Fig. 11.1
We routinely mark the pisiform and draw the anticipated path of the median nerve (dotted line), which is directly beneath or slightly ulnar to the palmaris longus tendon (if present). The flexor carpi radialis should be easily palpable in most patients and serves as the radial extent of the median nerve’s path, with the most ulnar aspect typically at the level of the flexor tendons
Fig. 11.2
Our proximal incision is centered to slightly radial over the median nerve. We choose to place it just proximal to the distal wrist flexion crease for patient comfort postoperatively. The distal, or palmar, incision is placed at the junction of a line connecting the fully radially abducted thumb and the hamate hook and a line drawn from the radial aspect of the ring finger
11.8.4 Procedure
Figures 11.3, 11.4, 11.5, 11.6, 11.7, 11.8, 11.9, 11.10, 11.11, 11.12, 11.13, 11.14, 11.15, 11.16, 11.17, 11.18, 11.19, and 11.20 illustrate the rest of the procedure.
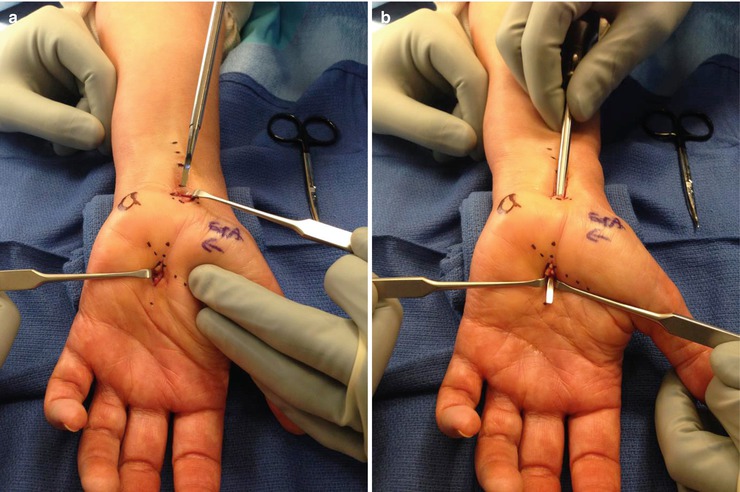
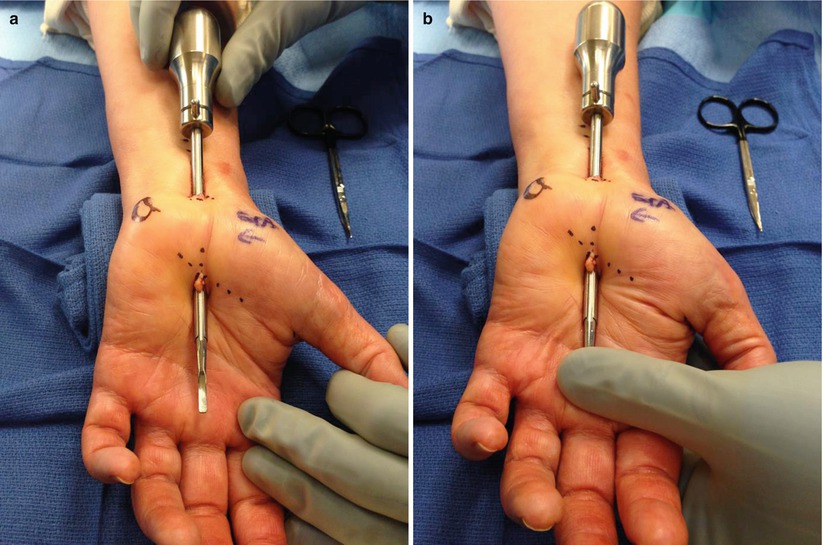
Fig. 11.3
Utilizing a #15 blade, the proximal skin is incised with dissection through the superficial tissue, in line with the median nerve, using a blunt tenotomy scissors to the antebrachial fascia
Fig. 11.4
Two medium smooth retractors aid the superficial retraction. The palmaris longus, if present, is retracted radially to protect the palmar cutaneous branch of the median nerve. A third retractor retracts the proximal skin to expose the antebrachial fascia for incision
Fig. 11.5
A separate (deep) #15 blade is used to create an opening in the antebrachial fascia. The blunt tenotomy scissors are used to safely complete the proximal release of the antebrachial fascia. The scissors are directed proximally and slightly ulnarward, to protect the palmar cutaneous branch of the median nerve. The fascia is released for 2–3 cm
Fig. 11.6
A Chow elevator is inserted into the carpal tunnel at approximately a 45° angle through the proximal opening to create a path for the camera trocar. The elevator should be inserted carefully to avoid violation of the median nerve, which is easily visualized. The tip of the elevator is used to brush the undersurface of the transverse carpal ligament, creating a “washboard” sensation. Occasionally, in chronic cases of carpal tunnel syndrome, the transverse carpal ligament is adherent to the underlying contents, in which case the Chow elevator can be used to gently free the undersurface of the ligament
Fig. 11.7
Once the Chow elevator has traversed the extent of the ligament, the tip is palpable at the palmar incision. Palpation of the elevator tip distal to the previously marked incision should be carefully evaluated, as the superficial palmar arch will be in close proximity. Extending the wrist will displace the arch dorsally, protecting it from injury
Fig. 11.8
(a–c) Distal incision is made with the “skin” #15 blade with dissection in line with palmar fascia, using the Stevens tenotomy scissors to create a path for the Chow elevator to be delivered through the distal surgical site. To decrease the chance of injury to the palmar arch, two medium smooth retractors aid in visualizing the tip of the Chow elevator as it is delivered distally
Fig. 11.9
(a, b) Leaving one medium smooth retractor in the distal site and moving one to the proximal site, the slotted camera trocar with obturator is inserted beneath the transverse carpal ligament, using the obturator tip to “scrub” the undersurface of the ligament as previously done with the Chow elevator. As the obturator tip approaches the palmar incision, both medium smooth retractors protect the palmar arch by aiding its delivery
Fig. 11.10
Once the trocar has been delivered through the palmar incision (a), a thumb should be placed in the curved end of the obturator (b) to control the rotation of the trocar while the hand is positioned on the endoscopic platform
Fig. 11.11
The extremity is placed on the endoscopic platform with the elbow flexed to approximately 45° and the wrist extended to 70° (or the patient’s comfort level). A strap is placed over the fingers to allow instrument insertion through each end of the trocar
Fig. 11.12
 Endoscopic Harvest of the Fascia Lata for Facial Reanimation
Endoscopic Harvest of the Fascia Lata for Facial Reanimation
 Video-Assisted Thoracoscopic Sympathicotomies for the Treatment of Palmar and Axillary Hyperhidrosis
Video-Assisted Thoracoscopic Sympathicotomies for the Treatment of Palmar and Axillary Hyperhidrosis
 Endoscopic Diastasis Recti Repair
Endoscopic Diastasis Recti Repair
 Endoscope-Assisted Brow Lift
Endoscope-Assisted Brow Lift
 Transaxillary Endoscopic Subfascial Breast Augmentation
Transaxillary Endoscopic Subfascial Breast Augmentation
 Endoscopic Flap Design and Harvesting
Endoscopic Flap Design and Harvesting




Related posts:
Endoscopic Harvest of the Fascia Lata for Facial Reanimation
Video-Assisted Thoracoscopic Sympathicotomies for the Treatment of Palmar and Axillary Hyperhidrosis
Endoscopic Diastasis Recti Repair
Endoscope-Assisted Brow Lift
Transaxillary Endoscopic Subfascial Breast Augmentation
Endoscopic Flap Design and Harvesting
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
