where V m is the transmembrane potential, ƒ is a function describing the electrical and geometrical properties of the cell, E is the strength of applied electric field, r is the cell radius, and θ is the polar angle with respect to the direction of the external field. Many researchers list the value of ƒ as 1.5 (Kotnik et al. 1997, 1998). Electroporation is attained when V m is greater than the threshold potential (V s ). As the bilayer cell membrane is a common feature for eukaryotic cells, the value of V s is comparable to different cell types and is reported to be 1 V (Kinosita and Tsong 1977b). However, the theoretical and experimental study conducted by Teissie and Rols (Teissie and Rols 1993) described Vs as being 200 mV. Therefore, a pulse voltage of 20–40 V (about 250–500 mV/bilayer) is sufficient to achieve short-term permeabilization of multilayer SC (~70–100 lipid bilayers) (Gallo et al. 1997; Pliquett et al. 1995). For prolonged permeabilization of the SC, a pulse voltage higher than 75 V (1 V/bilayer) is required.
7.2.1 Expansion of Preexisting Pathways
A schematic drawing of the SC with the possible pathways of transport during electroporation is shown in Fig. 7.1. At relatively low voltages (<30 V across the skin), the drop in skin resistance and enhanced transdermal transport can be mainly attributed to electroporation of the appendageal ducts present in the skin (Chizmadzhev et al. 1998). However, electroporation of the appendageal ducts does not show dramatic increase in the transdermal transport of molecules (Chen et al. 1998). At higher voltages (>30 V), electroporation of the lipid-corneocyte matrix leads to an additional drop in skin resistance, which allows dramatic increase of the drug transport (Chen et al. 1998; Weaver et al. 1999).
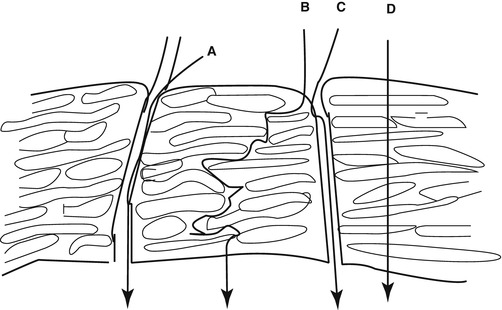
Fig. 7.1
Schematic drawing of the stratum corneum with the possible pathways (preexisting and new) of transport during electroporation. Preexisting pathways include (A) via hair follicle; (B) via intercellular, involving the gaps between corneocytes; (C) via sweat ducts and (D) newly created due to electroporation pathway that goes through the corneocytes and lipid bilayers
7.2.2 Creation of New Pathways
Application of electric pulses of high voltage to the skin results in a dramatic increase of transdermal transport associated with reversible structural changes in the skin (Prausnitz et al. 1993a) which causes permeabilization of the SC and is generally believed to occur through the formation of aqueous pathways across the lipid bilayers of the SC. Electroporation alters lipid bilayers when transient electric field leads to the formation of non-lamellar lipid phases: a pore, also called localized transport region (LTR). These new aqueous pathways are thought to be formed when the water from both sides of the membrane meets due to the electric field force (Pliquett 1999). The pore mechanism for the enhanced transdermal transport is generally accepted. In addition to electroporation, the local electric field also provides a driving force for the small ions and water-soluble molecules to traverse the skin through these newly created pathways (Vaughan and Weaver 2000).
7.2.3 Thermal Effects Due to Electroporation
When electrical energy passes through a resistance, it is transformed into heat. According to the first law of thermodynamics, the electrical energy released into a system will increase the energy level of the sample. Thus, the heat production due to electrical energy dissipation results in an increase in the sample temperature. However, the increases in the temperature are not drastic as the whole circuit is involved in the energy dissipation, not just the sample (Lurquin 1997). Nevertheless, caution should be observed when multiple pulses of longer duration are applied. It is hypothesized that the application of electric pulses causes temperature rise in the SC during electroporation, which might further contribute to permeation enhancement. It was estimated by computer simulation that for a peak voltage of 70 V exponential decay pulse across the SC, the temperature rise would be 19 °C (Martin et al. 2002). These temperature rises occurred within localized regions surrounding the LTRs and are called localized dissipation regions (LDRs) (Pliquett et al. 2002; Weaver et al. 1998). The morphological changes studied using time-resolved freeze-fracture electron microscopy following electroporation revealed the formation of multilamellar vesicles of 0.1–5.5 nm in diameter in the intercellular lipid bilayers of the SC (Gallo et al. 1999). These vesicles were similar to those formed when the SC is heated to 65 °C, suggesting that these changes are related to the heating effect of the electric pulses (Gallo et al. 1999). The temperature rise within SC may alter the structure and prolong the recovery of the skin barrier after electroporation (Murthy et al. 2004).
7.2.4 Molecular Transport Mechanisms
Diffusion, electrophoretic movement, and electroosmosis are the major mechanisms of molecular transport through temporary permeabilized skin by electroporation (Tien and Ottova 2003). While diffusion plays a major role in the permeation of small uncharged molecules (Tekle et al. 1994), electrophoretic movement is the main driving force for the transport of charged macromolecules such as DNA (Prausnitz et al. 1993a; Regnier et al. 1999). Although diffusion can occur during and after pulse application, electrophoresis is evident only during pulse application (Escobar-Chavez et al. 2009). In contrast to iontophoresis, the use of short-time electric pulse limits the contribution of electroosmosis in drug permeation by skin electroporation. The impact of diffusion and electrophoresis depends on the physicochemical properties of the drug such as geometric size, shape, and charge (Chen et al. 2006).
7.3 Factors Influencing Percutaneous Penetration Enhancement by Electroporation
There are several parameters influencing the extent of percutaneous penetration enhancement of drug molecules using electroporation. These include both electrical parameters associated with the pulses and physicochemical properties of the molecules to be delivered.
7.3.1 Electrical Parameters
7.3.1.1 Types of Pulses
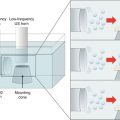
Two different types of pulses (wave forms), square-wave (Denet and Préat 2003; Medi and Singh 2003) and exponentially decaying (Chang et al. 2000; Prausnitz et al. 1993a), are being investigated for percutaneous penetration enhancement (Fig. 7.2). Square-wave pulse electroporators generate a voltage pulse using fast switches. Basically, the power supply set to generate a given voltage is connected to a square-wave pulse generator, which closes the circuit at t = 0 and opens it at a defined time point later. Thus, the theoretical shape of the wave is as shown in Fig. 7.2a. Square-wave pulses do not rely on capacitor discharge into the circuit as in the case of exponential decay pulses. Hence, square-wave electroporation permits the use of multiple pulses of fixed voltage for a constant period of time (Golzio et al. 1998; Jordan et al. 2008). It has been reported that higher gene transfection efficiencies can be achieved when square-wave electroporation is utilized to transfer DNA into cells (Liu and Bergan 2001; Takahashi et al. 1991). However, during exponential decay wave forms (Fig. 7.2b), an initial pulse voltage is selected, and the duration of the decay depends on the capacitance setting of the electroporation system and the resistance of the skin. Therefore, the reproducibility of exponential decay pulse conditions for clinical application might be problematic, while this is not an issue with square-wave pulses (Denet et al. 2004). Nevertheless, skin electroporation using exponentially decaying pulses was shown to be more effective (Fig. 7.3). Due to its long voltage tail, exponential decaying pulses can expand or maintain the high-permeability state of the skin for a prolonged period of time to facilitate the electrophoretic mobility of drugs (Vanbever et al. 1996).
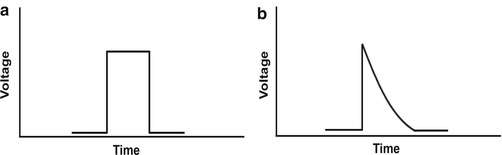
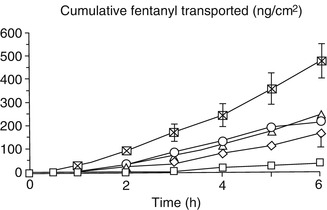
Fig. 7.2
Schematic drawing of the (a) square-wave and (b) exponential decay pulses. The electrical pulse parameters, especially the duration of the pulses, can be better controlled in the case of square-wave pulse than in exponentially decaying pulses
Fig. 7.3
Effect of the type of electroporation pulses applied on cumulative transport of fentanyl through full-thickness hairless rat skin. Key: (□) passive diffusion, (◊) 5 × (100 V–60 ms) square-wave pulses, (○) 5 × (250 V–60 ms) square-wave pulses, (△) 5 × (100 V–125 ms) exponentially decaying pulses, (☒) 5 × (250 V–125 ms) exponentially decaying pulses. Fentanyl 40 μg/ml was introduced in a citrate buffer pH 5 (0.01 M) (Reproduced from Vanbever et al. 1996. With permission of Springer)
7.3.1.2 Pulsing Parameters
The pulsing parameters, such as pulse amplitude, pulse length, number of pulses, and the interval between each pulse, can have a dramatic effect on the transport of drugs through the skin during electroporation. Pulse amplitude is reported to be a critical parameter, which has a profound effect on the transdermal delivery of drugs (Zorec et al. 2013). Sharma et al. (2000) reported that the transport of terazosin hydrochloride through hairless rat skin was enhanced linearly with pulse amplitude using exponentially decaying pulses. In another study human parathyroid hormone (1–34), hPTH (1–34), delivery was shown to depend linearly on the pulse amplitude using square-wave pulses (Fig. 7.4) (Medi and Singh 2003). The pulse length and number of pulses also affect the extent of transdermal delivery as shown in Figs. 7.5 and 7.6, respectively. The pulsing frequency might also play an important role as the large number of pulses with a big time gap between them may not be useful, which allows the recovery of skin barrier before the application of the next pulse.
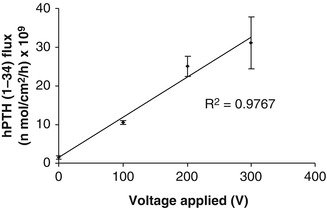
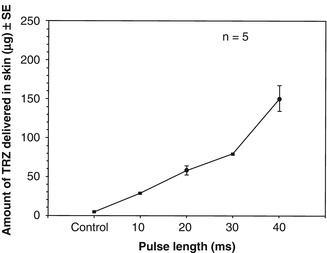
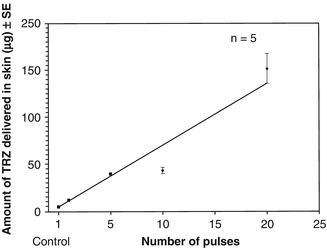
Fig. 7.4
Effect of electroporation pulse voltages on the flux of hPTH (1–34) through dermatomed porcine skin. Twenty square-wave pulses of 100 ms pulse length with 1 s interval between each pulse and of different voltage were applied at the beginning. Pulses were applied to 0.785 cm2 area of the skin. Values are shown as the mean ± SD of three determinations (Reproduced from Medi and Singh 2003. With permission of Elsevier)
Fig. 7.5
Effect of pulse length on terazosin hydrochloride (TRZ) delivery. Twenty pulses at 88 V were delivered using small-area electrode (Reproduced from Sharma et al. 2000. With permission of John Wiley and Sons)
Fig. 7.6
Effect of number of pulses on TRZ delivery. The voltage was set at 88 V and the pulse length was set at 40 ms (Reproduced from Sharma et al. 2000. With permission of John Wiley and Sons)
7.3.1.3 Electrode Design
Since the intensity and distribution of the electrical field can be significantly affected by electrode geometry and their position throughout the pulse application, the efficiency of drug transport is greatly influenced by the proper selection of electrodes and their positioning with respect to the tissue to be electroporated (Kanduser and Miklavcic 2008). For use in medicine, electrode design has to allow both efficient drug/gene transport and maximum protection of the surrounding tissue from cell damage.
The electrodes used for skin electroporation can be classified into two major groups: noninvasive electrodes and invasive electrodes. The most common noninvasive electrode consists of two parallel plate electrodes with either fixed or variable distances positioned around the injected sample. Although simple plate electrodes are often used in a clinical setting for the treatment of cutaneous and subcutaneous metastases, they can cause superficial skin burning and stimulation of underlying muscles and nerves (Denet et al. 2004). The use of a meander electrode can protect the underlying tissue from undesirable side effects since its electric field is mostly localized within the superficial skin layers (Denet et al. 2004). Heller et al. (2007) have designed a special type of plate electrode (4PE) consisting of four plates to deliver electric pulses in two different orientations perpendicular to each other. This electrode design provides easier and more reproducible cutaneous plasmid delivery than commercially available simple plate electrodes. Other commonly used noninvasive electrode types are contact wires (Heller et al. 2001; Mazères et al. 2009; Pedron-Mazoyer et al. 2007), flat patch electrode (Babiuk et al. 2003; Heller et al. 2010; Zhang et al. 2002), and tweezers electrode. In the case of contact wire electrodes, the sample is injected between the two wires, while the flat patch electrode is placed directly on the injected sample.
The invasive electrodes comprise of various needle configurations, either in circular or pair-wise array. They are generally used for the treatment of tumors or vaccinations. Invasive electrodes are inserted near the periphery of the injection site to avoid any leakage of the sample. Maruyama et al. (2001) made a special type of electrode design where the needles were inserted into the skin parallel to the body surface, rather than conventional vertically directed electrodes. In another study, Daugimont et al. (2010) used hollow conductive microneedle arrays for the intradermal delivery of drugs and DNA. This microneedle array played a dual role in allowing needle-free intradermal injection of the sample as well as for electric pulse application in the superficial skin layers.
Since most of the skin permeation studies by electroporation have been executed in rodents, noninvasive electrodes have been used frequently. However, several studies conducted in large animals, such as pigs which have relatively thicker skin, showed the superiority of needle electrodes over conventional plate electrodes (Drabick et al. 2001). Therefore, the selection of the most suitable electrodes and their design depends upon both the purpose of electroporation as well as the characteristics of the treated cells.
7.3.2 Physicochemical Factors
7.3.2.1 Molecular Size and Charge of the Permeant
The size and charge of the drug molecule play an important role in percutaneous absorption. Figure 7.7 shows the effect of molecular weight (MW) of the permeant on the transdermal transport using electroporation, i.e., an increase of MW causes a decrease of the transport. Since the electrophoretic movement is the primary transport mechanism for charged macromolecules through the skin by electroporation, both the pKa of the permeant and the pH of the delivery formulation play a critical role in the overall absorption process. The general rule is that the higher the charge of the permeant, the greater the absorption potential (Denet et al. 2004). Electroporation has shown a 5–10,000-fold increase in the flux of calcein (Prausnitz et al. 1993a), luteinizing hormone-releasing hormone (LHRH) (Bommannan et al. 1994), heparin (Prausnitz et al. 1995), oligonucleotides (Regnier et al. 1998), fluorescein isothiocyanate (FITC)-labeled dextran (Lombry et al. 2000), insulin (Sen et al. 2002a), and hPTH (1–34) (Medi and Singh 2003). These studies suggest that electroporation can be useful for the transdermal delivery of macromolecules that could not be transported using other enhancement methods.
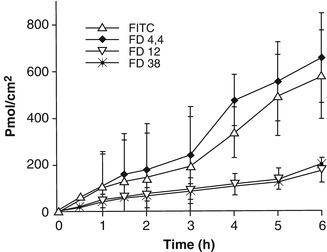
Fig. 7.7
Effect of molecular weight of permeant on cumulative transdermal transport using electroporation. Ten (150V–150 ms, each separated by 30 s) exponentially decaying pulses were used to measure the transport of FITC-dextran (FD) of increasing molecular weight (4.4, 12, and 38 kDa) across hairless rat skin in vitro. (Reproduced from Lombry et al. 2000. With permission of Springer)
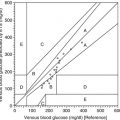
7.3.2.2 pH of the Formulation
The pH of the formulation is also an important factor that can influence the barrier properties of the skin in addition to its influence on the ionic state of the drug. Enhanced percutaneous penetration of water without electroporation was reported at pH lower than 4 and higher than 10 due to the extraction of the insoluble fraction of keratin (Matoltsy et al. 1968). The electrical impedance of the skin was also found to be decreased at a pH lower than 3 and higher than 9 (Allenby et al. 1969). Murthy et al. (2003) showed the pH dependence of the electroporation-enhanced transport using glucose and FITC-labeled dextran (FD). They reported that the transport of glucose and FD across porcine epidermis was increased by three-fold when the formulation pH was increased from pH 5 to 7.5, which might be due to the prolonged postpulse permeability state of the skin.
7.3.2.3 Effect of Electrolytes
The presence of monovalent electrolytes such as NaF, NaCl, NaBr, and NaI (Fig. 7.8) and divalent electrolytes such as MgCl2 and CaCl2 (Fig. 7.9) was shown to have a synergistic effect on the electroporation-enhanced transport of calcein across the hairless rat skin (Tokudome and Sugibayashi 2003). The presence of CaCl2 was shown to prolong the postpulse recovery of the skin, which might be the reason for the enhanced transport in comparison to electroporation alone (Tokudome and Sugibayashi 2004). Simultaneous application of these electrolytes and electroporation caused 10–83-fold enhancement in the skin permeation of calcein compared to electroporation alone.
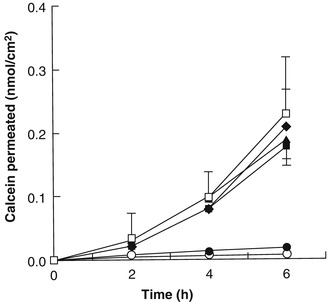
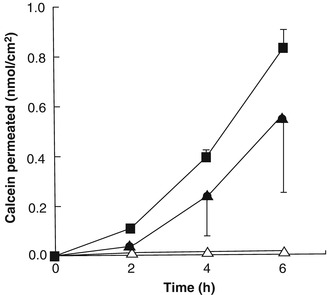
Fig. 7.8
Effect of various monovalent electrolytes on electroporation-enhanced permeation of calcein through excised hairless rat skin. Symbols: ○, control (passive diffusion); •, distilled water; ♦, NaF; ■, NaCl; □, NaBr; ▲, NaI (Reproduced from Tokudome and Sugibayashi 2003. With permission of Elsevier)
Fig. 7.9
Effect of various divalent electrolytes on electroporation-enhanced permeation of calcein through excised hairless rat skin. Symbols: ○, control (passive diffusion); •, distilled water; ■, CaCl2; ♦, MgCl2; ▲, CuCl2; Δ, ZnCl2. Each point represents the mean ± SE of three to five determinations (Reproduced from Tokudome and Sugibayashi 2003. With permission of Elsevier)
7.3.2.4 Effect of Temperature
It is well known that temperature affects the permeability of the diffusing drug molecules through the skin (Oh et al. 1993; Peck et al. 1995). It has been shown that an increase in temperature above 40 °C results in enhanced transport of molecules with electroporation (Fig. 7.10), which is likely due to the delayed recovery of the skin following electroporation (Murthy et al. 2004).
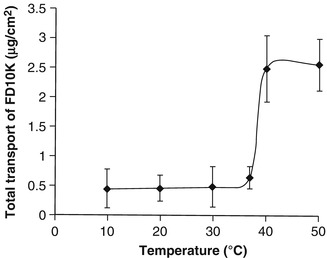
Fig. 7.10
Total electroporation transport of FD10K across porcine epidermis at different temperatures. Porcine epidermis samples were subjected to 60 pulses, each of 1-ms duration at 100 V, 1 Hz. FD10K (5 mg/mL) was present in the donor chamber during the pulse application and for 15 min after pulsing (Reproduced from Murthy et al. 2004. With permission of John Wiley and Sons)
7.4 Effects of Electroporation on Skin
In order to be useful clinically, the permeabilization of SC should be reversible as it is the primary barrier between the body and the environment besides playing a critical role in regulating the homeostatic reactions. Unlike electroporation of simple lipid bilayers, which anneal immediately after ceasing the pulses, the complex lipid matrix of the SC has a slower return to normal permeability state (Riviere and Heit 1997). Although not completely understood, application of strong electric pulses to cells and tissues is known to cause some type of structural rearrangement of the cell membrane due to the combined electrical and thermal effects (Pliquett et al. 2002; Weaver 1995). In most of the cases, the overall changes to the skin following electroporation are mild and reversible.
Since the SC layer has much higher electrical resistance than underlying tissues, the applied electric field to the skin will initially concentrate in the SC and could provide efficient protection from adverse effects to the underlying viable tissues. However, upon the application of a high-voltage electric pulse, SC’s resistance drops dramatically to permit the greater extent of electric field into the deeper tissues, causing direct excitation of the underlying nerves and muscles (Prausnitz 1996). An increase in pulse voltage, duration, and rate is likely to intensify the sensation of itching, pricking, tingling, muscle contractions, and pain (Denet et al. 2004). These unwanted side effects could be avoided by the use of closely spaced microelectrodes that confine the electric field to SC layer (Pliquett and Weaver 2007). The present section delineates the studies carried out so far to address the safety issues using electroporation.
7.4.1 Biophysical Changes
The lipid structure of SC is known to undergo several structural rearrangements at elevated temperatures during electroporation. Although these temperatures may slightly differ for various animal species, the SC experiences roughly four endothermic phase transitions over a temperature range of 40–130 °C (Becker 2012). The phase transition that occurs within the temperature range of 60–70 °C greatly destabilizes the SC’s lipid barrier function and is primarily attributed to the disordering of the lamellar lipid phase (Cornwell et al. 1996). Biophysical methods allow investigators to study the changes of SC lipids and proteins in addition to the SC water content. Different methods including Fourier transform infrared spectroscopy (FTIR), differential thermal analysis (DTA), differential scanning calorimetry (DSC), and X-ray diffraction have been used to investigate these changes following electroporation treatment. Attenuated total reflectance (ATR)-FTIR studies show an increase in the water content of SC (Jadoul et al. 1999), which was also confirmed by thermogravimetric studies (Jadoul et al. 1998b). A dramatic perturbation in the lamellar ordering of the intercellular lipid has been reported after high-voltage pulsing using differential thermal analysis and freeze-fracture electron microscopy (Jadoul et al. 1998b). Polarized light thermal microscopy of extracted lipids from the SC shows an indication of overall lipid structure fluidization around 60 °C (Silva et al. 2006). Small-angle X-ray scattering studies carried out about 5 min after electroporation pulsing provided further evidence for a general perturbation of interlamellar and intralamellar lipid packing order (Jadoul et al. 1997).
7.4.2 Histological Changes
Electroporation-induced skin damage is often assessed histologically after staining with hematoxylin and eosin (Heller et al. 2008). Histological examination of the skin after electroporation showed intraepidermal edema, focal vacuolization, and degeneration of the epidermal layer (Guo et al. 2011; Riviere et al. 1995). An increased detachment of SC cell layers and an amorphous epidermis (Fig. 7.11) were reported with an increase in electroporation pulse voltage (Jadoul et al. 1998b; Medi and Singh 2003). Freeze-fracture electron microscopic studies revealed a severe distortion of the lamellar structure of the SC lipids (Jadoul et al. 1998b). Another study using time-resolved freeze-fracture electron microscopy revealed the formation of multilamellar vesicles of 0.1–5.5 nm in diameter in the SC that could be related to the heating effect of electroporation (Gallo et al. 1999).
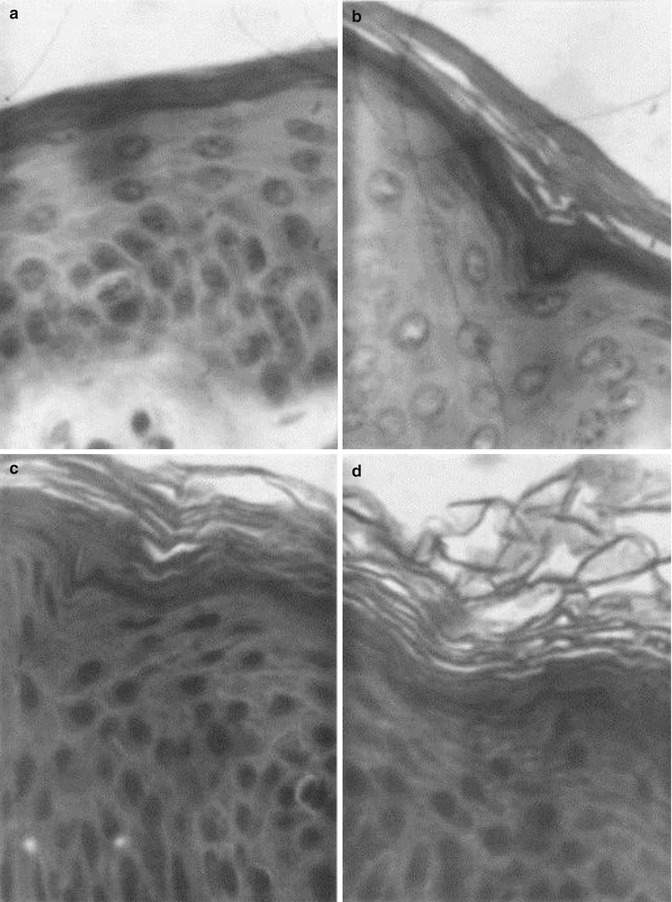
Fig. 7.11
Effect of electroporation on skin. (a) Microscopic section of control porcine skin (without any electric pulses), (b) microscopic section of skin sample electroporated with pulses of 100 V, (c) microscopic section of the skin treated with pulses of 200 V, and (d) microscopic section of the skin treated with pulses of 300 V. Images were taken at 100× magnification (Reproduced from Medi and Singh 2003. With permission of Elsevier)
7.4.3 Macroscopic Barrier and Skin Irritation
The barrier property of the skin is critical to prevent the entry of exogenous toxic chemicals into the body and also to avoid the loss of internal body components, particularly water (Roberts and Walters 1998). The effect of electroporation on the macroscopic barrier property of the skin was studied by measuring transepidermal water loss (TEWL) following electroporation in vivo in rats and rabbits (Dujardin et al. 2002; Medi and Singh 2006; Wang et al. 2007). The studies reported a reversible increase in TEWL following electroporation. It is shown to cause mild, transient erythema and edema in New Zealand white rabbits (Medi and Singh 2006). Skin irritation was measured at different time points following the visual scoring method of Draize et al. (1944). It is suggested that the use of iontophoresis followed by electroporation pulses might reduce the skin irritation (Prausnitz et al. 1993b; Vanbever et al. 1998a). This may be due to the creation of new pathways with electroporation, which results in more even distribution of the iontophoretic current (Singh and Maibach 2002). A recent study using a surface electroporation device demonstrated the effect of pulse voltage on the dermal integrity of guinea pig skin (Broderick et al. 2012). At the 48 h time point, skin sites treated with 200, 100, and 50 V electric pulses showed signs of redness and swelling. In addition, 200 and 100 V electric pulse treatments also showed signs of inflammation and scabbing, while the skin site treated with 10 V pulses did not show visible signs of tissue damage. On the contrary, electroporation of the guinea pig skin using a noninvasive multielectrode array (250 V/cm, 150 ms) demonstrated no sign of severe skin damage such as burning, ulceration, or scar formation (Guo et al. 2011). Only skin redness and prints of the electrodes were observed after electroporation and disappeared by day 5. Some transient hair loss was evident in the site of electroporation, but it grew back within 7 days of treatment. Thus, the selection of proper voltage parameters and electrodes is important to carry out safe and effective electroporation.
7.5 Potential Applications
Electroporation is an attractive physical technique, because it offers a simple, effective means of facilitating the permeation of a wide range of exogenous molecules across the skin by transiently disrupting the cell membrane. Moreover, for in vivo application, the area of tissue affected by electroporation can be effectively controlled or confined by the appropriate localization of applied electric field (Esser et al. 2009; Pliquett et al. 2004). The encouraging results of in vitro electroporation studies persuade researchers to investigate the potential of electroporation-based medical therapies. The current in vivo application of electroporation encompasses drug delivery (Tokumoto et al. 2006; Wong et al. 2006), gene delivery (including DNA vaccination) (Luckay et al. 2007; Medi et al. 2005; Wells et al. 2000), or electroporation alone (without any therapeutically active molecules) for tissue ablation (Al-Sakere et al. 2007). A number of studies have demonstrated that electroporation could be used to enhance the delivery of impermeant anticancer drugs to the solid tumor tissue (Gothelf et al. 2003; Mir and Orlowski 1999). More interestingly, recent studies have reported that the use of very short duration and higher-voltage electric pulses can irreversibly destroy the target cells within a limited area while leaving adjacent cells unaffected (Lee et al. 2010). This provides a new opportunity for the treatment of cancer, cardiovascular diseases, and other ailments that necessitate removal of tissue. This section emphasizes the use of electroporation for transdermal drug and gene delivery.
7.5.1 Transdermal or Topical Drug Delivery
Since the demonstration of the electroporation for enhanced transdermal delivery (Prausnitz et al. 1993a), numerous studies reported the delivery of several molecules. It can improve transdermal/topical delivery of drugs ranging from small molecules to macromolecules such as peptides and nucleic acids (oligonucleotides and genes). Enhanced transdermal delivery of macromolecules of at least up to 40 kDa was shown to be feasible with electroporation. Table 7.1 provides a summary of the percutaneous penetration enhancement of different drugs using electroporation.
Table 7.1
Summary of percutaneous penetration enhancement of drugs using electroporation
Drug | Electroporation protocol | Membrane | Enhancement | Reference(s) |
|---|---|---|---|---|
5-fluorouracil | Twenty ED pulses of 300 V, 200 ms long
Related posts: Microporation in Penetration Enhancement Microporation in Penetration Enhancement
 Combined Use of Ultrasound and Other Physical Methods of Skin Penetration Enhancement Combined Use of Ultrasound and Other Physical Methods of Skin Penetration Enhancement
 Gene Transfer to the Skin by Physical Methods of Delivery Gene Transfer to the Skin by Physical Methods of Delivery
 Magnetophoresis: Skin Penetration Enhancement by a Magnetic Field Magnetophoresis: Skin Penetration Enhancement by a Magnetic Field
 Therapeutic Applications of Electroporation Therapeutic Applications of Electroporation
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|