Eave Skin Flap for Helical Reconstruction
M. L. LEWIN
EDITORIAL COMMENT
This is an important principle not only in ear reconstruction, but at other sites in the body where one flap is required to fold into another flap, such as in alar-base reconstruction.
The helix is the most prominent part of the external ear, visible when viewing the face from the front and even more conspicuous in profile. The most frequent deformity of the helix occurs in facial burns. Because of its prominence and its thin skin and cartilage, the helix is often destroyed, leaving the auricle with a flat, scarred, jagged rim (Figs. 80.1A and 80.2A). Other helical deformities are due to lacerations, excision of tumors, or harvesting of large composite grafts (1).
INDICATIONS
If the helical defect is small, it is best repaired by a chondrocutaneous flap, but if the defect is larger than 2.5 cm, this procedure will reduce the size of the auricle. Several procedures are recommended for reconstruction of the helix. Some may require multiple stages, may leave conspicuous scars, or are applicable only to small helical losses.
The eave skin flap was devised primarily for isolated defects of the helix (2). It can be used to reconstruct the entire helix or a portion of it (3) in a two-stage procedure that can be performed with the patient under local anesthesia without hospitalization. It uses the postauricular and mastoid skin, which is a good match for the skin of the ear. The flap donor-site scar or skin graft is concealed behind the ear.
In assembling the cartilaginous framework in total ear reconstruction provision is made for the helix. A vertical strip of cartilage extends above the horizontal plane of the scapha; however, the skin flap that covers the cartilaginous framework frequently effaces the prehelical sulcus so that the helical outline is lost. An eave flap can restore the sharp delineation of the helix. The eave flap is not advised when the ear framework is of alloplastic material.
FLAP DESIGN AND DIMENSIONS
The procedure is based on the observation that a skin flap that is dissected free and held at both ends will curl until it spontaneously tubes itself. This curling is caused by the contracture of the denuded undersurface of the flap. If half the width of the flap is inserted into the tissue and the other half is unattached, the latter will curl until its undersurface becomes completely epithelialized.
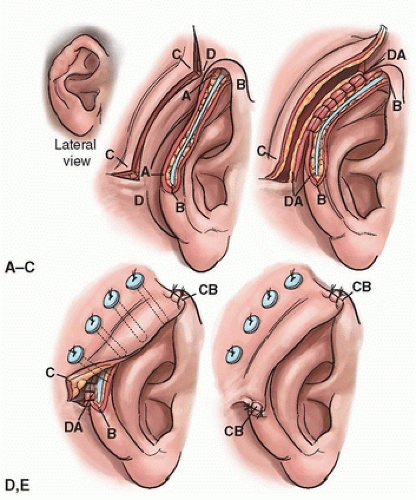 FIGURE 80.1 Diagram of procedure (see text). A: Preoperative appearance. B: Helical defect denuded by excision of marginal scar. The mastoid flap is incised. C: Formation of postauricular skin tunnel. D: Mastoid flap overlapping helical defect like an eave. E: Postoperative appearance. (From Lewin, ref. 2, with permission.)
Related posts: Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
 Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction
 Inferior Turbinate Flap for Closure of Septal Perforations Inferior Turbinate Flap for Closure of Septal Perforations
 Postauricular and Retroauricular Scalping Flap (The Paras Flap) Postauricular and Retroauricular Scalping Flap (The Paras Flap)
 Scapular and Parascapular Flaps Scapular and Parascapular Flaps
 Platysma Musculocutaneous Flap to The Lower Lip Platysma Musculocutaneous Flap to The Lower Lip
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|