24 Earlobe rejuvenation
Summary and Key Features
Anatomy and classification of earlobes
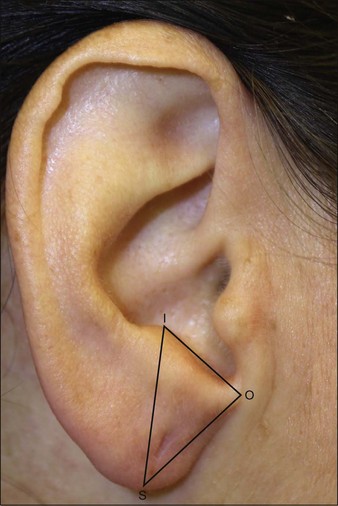
The earlobe is composed of tough areolar and adipose connective tissues and lacks the firmness and elasticity of the rest of the pinna. Earlobes have a tendency to elongate slightly with age. The surgery literature places an emphasis on repairing the elongated earlobe to complement the youthful face after a rhytidectomy. As early as 1972, Loeb recognized the potential need for earlobe rejuvenation. He described the distance between the intertragal notch and the otobasion inferius (the anterior implantation of the earlobe to the cheek skin) as a parameter requiring evaluation (Fig. 24.1). In his observations, he noted a range of 1–2.5 cm between the intertragal notch and the otobasion inferius (attached anterior segment; Fig. 24.1) and advocated correction when this distance exceeded 2.0 cm. A large study by Azaria et al (2003), which focused on the anatomy of the earlobe, used a line of balance through the long axis of the ear and measured the earlobe length based on the distance from the intertragic notch to the caudal tip (Fig. 24.2). The study consisted of 547 adult subjects ranging in age from 20 to 80 years. The subjects included 383 women (70%) and 164 men (30%). The average length of the left earlobe was 1.97 cm and that of the right earlobe 2.01 cm. From the data, the earlobes are naturally found to be slightly asymmetrical, which becomes clinically relevant so that the practitioner carefully assesses the size of each earlobe prior to treatment. Another study suggested that a complete assessment of earlobe height requires accounting for the entire lobule length as designated by its two components: the attached cephalic segment (the intertragal notch to otobasion inferius distance as described by Loeb), as well as its free caudal segment, which is the otobasion inferius to subaurale distance (see Fig. 24.1). Both measurements can be taken into consideration; however, it is more common to measure the earlobe length from the intertragal notch to the subaurale.