Preservation techniques have become more popular recently, in part due to the benefits of preserving normal nasal anatomy. There are preservation techniques that can be used to perform augmentation of the nose, including the nasal dorsum and middle nasal vault. These techniques involve the use of grafts placed below the nasal dorsum in the form of a subdorsal cantilever graft after releasing their attachments to the nasal skeleton. These techniques are complex and require experience in dorsal preservation and costal cartilage grafting. This article will discuss the use of the subdorsal cantilever graft for augmenting the nasal dorsum.
Key points
- •
Augmentation of the nose can be performed using preservation techniques incorporating a subdorsal cantilever graft.
- •
The subdorsal cantilever graft is positioned below the nasal dorsum to push up the nasal bones and middle vault.
- •
Subdorsal cantilever graft type A augments the middle vault and caudal nasal bones but does not elevate the radix.
- •
Subdorsal cantilever graft type B raises the radix as well as the nasal dorsum to augment the entire dorsum of the nose.
- •
The subdorsal cantilever graft is a complex graft that requires experience with dorsal preservation and costal cartilage grafting.
Video content accompanies this article at http://www.facialplastic.theclinics.com .
Introduction
Preservation rhinoplasty is a philosophy that focuses on preserving as much of the normal nasal anatomy as possible while modifying the shape of the nose. Preservation techniques highlight the preservation of the middle nasal vault, Pitanguy and scroll ligaments, and conservative tip maneuvers. Dorsal preservation focuses on preserving the structure of the middle nasal vault while reducing the dorsal hump. Using similar concepts, the nasal dorsum can be elevated or pushed up.
There are 2 main areas of augmentation that can employ the “push-up” techniques. In correction of the saddle nose deformity, the nasal bones are typically in proper position or may even exhibit a dorsal hump. In these cases, the middle vault is pushed up, and the nasal bones are managed as needed. In such cases, spreader grafts or other structural grafts can be placed below the middle vault to push up the depressed cartilages. These grafts must be very strong to support the middle vault and typically require autologous costal cartilage.
When performing major dorsal augmentation, as in the ethnic patient, a determination must be made on whether the radix needs to be raised in conjunction with the nasal dorsum or whether the radix position should remain the same, but the caudal nasal bones and middle vault elevated to align with increased tip projection.
This article covers preservation concepts used to correct the saddle nose deformity and augment the nasal dorsum.
Subdorsal cantilever graft
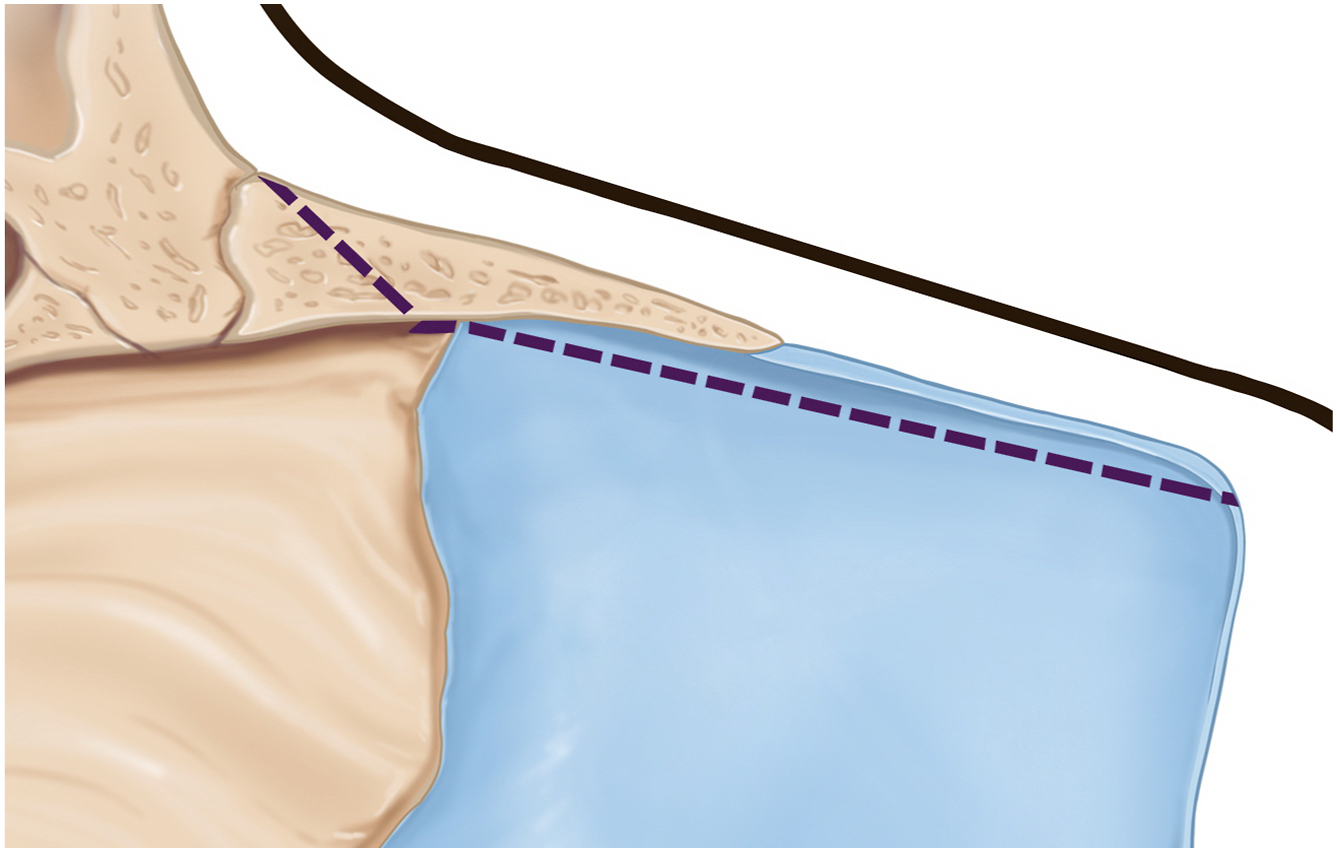
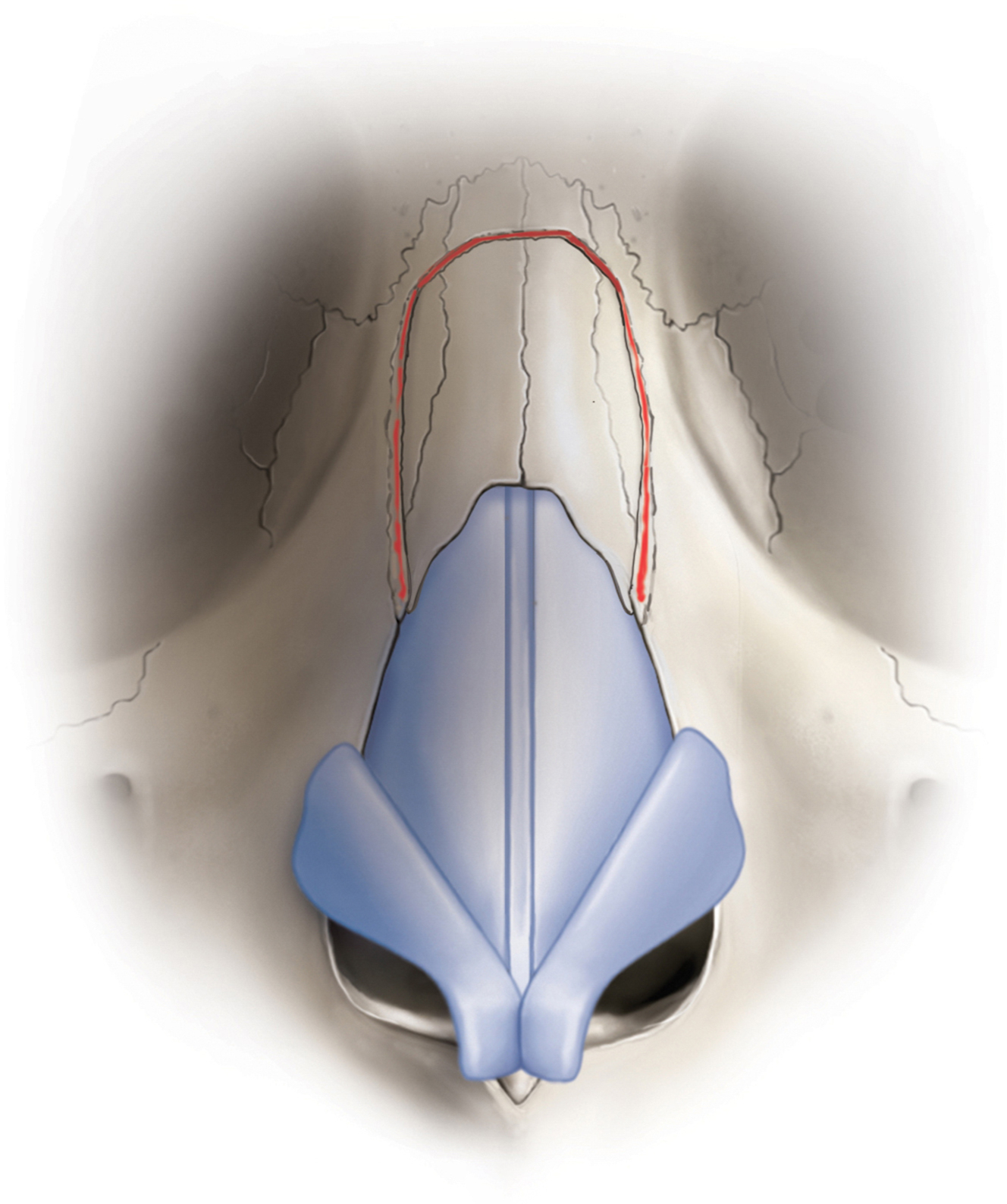
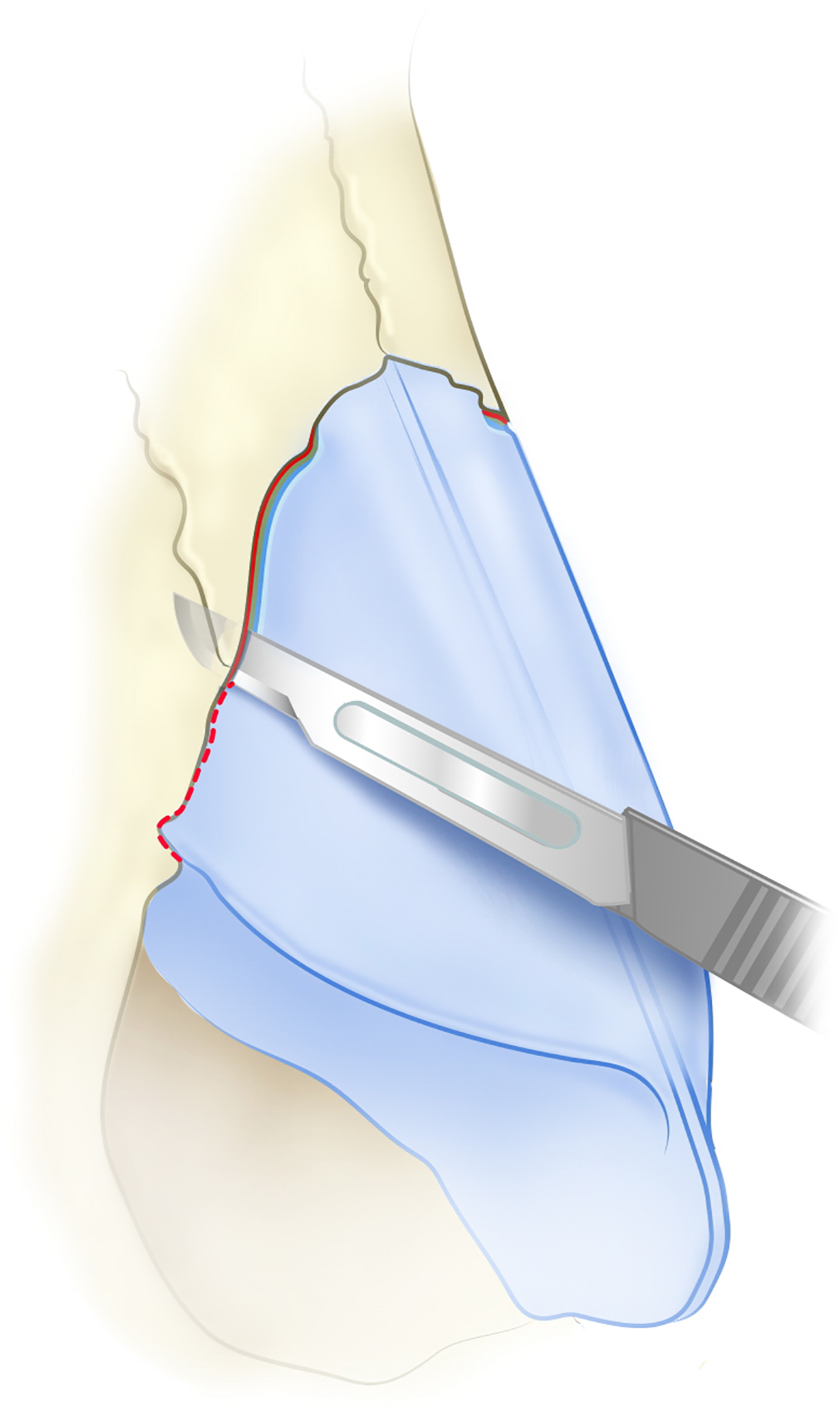
The subdorsal cantilever graft (SDCG) is a costal cartilage graft that can correct the saddle nose deformity and perform major dorsal augmentation. , There are 2 forms of the SDCG. Subdorsal cantilever graft type A (SDCG-A) is a single graft that extends from a space created under the bony nasal vault, passes under the middle vault, and then attaches firmly to a caudal septal extension graft or caudal septal replacement graft ( Fig. 1 ). The subdorsal space is created by incision in the septum immediately under the upper lateral cartilages, removing some bone under the nasal bones, and then allowing the middle vault and nasal bones to be pushed up from below ( Fig. 2 ). If the nasal bones need to be elevated, circumferential bone cuts can also be made to allow the bony vault to be pushed up ( Fig. 3 ). In order for the middle vault to push up, a complete lateral keystone release with division of the piriform ligament is needed ( Fig. 4 ). With the SDCG-A, the radix is not elevated, so a radix bone cut may not be necessary in many cases. In cases with shorter nasal bones, no bone cuts may be needed. With longer nasal bones, at least lateral osteotomies and transverse bone cuts will likely be necessary, creating a hinge point at the radix.
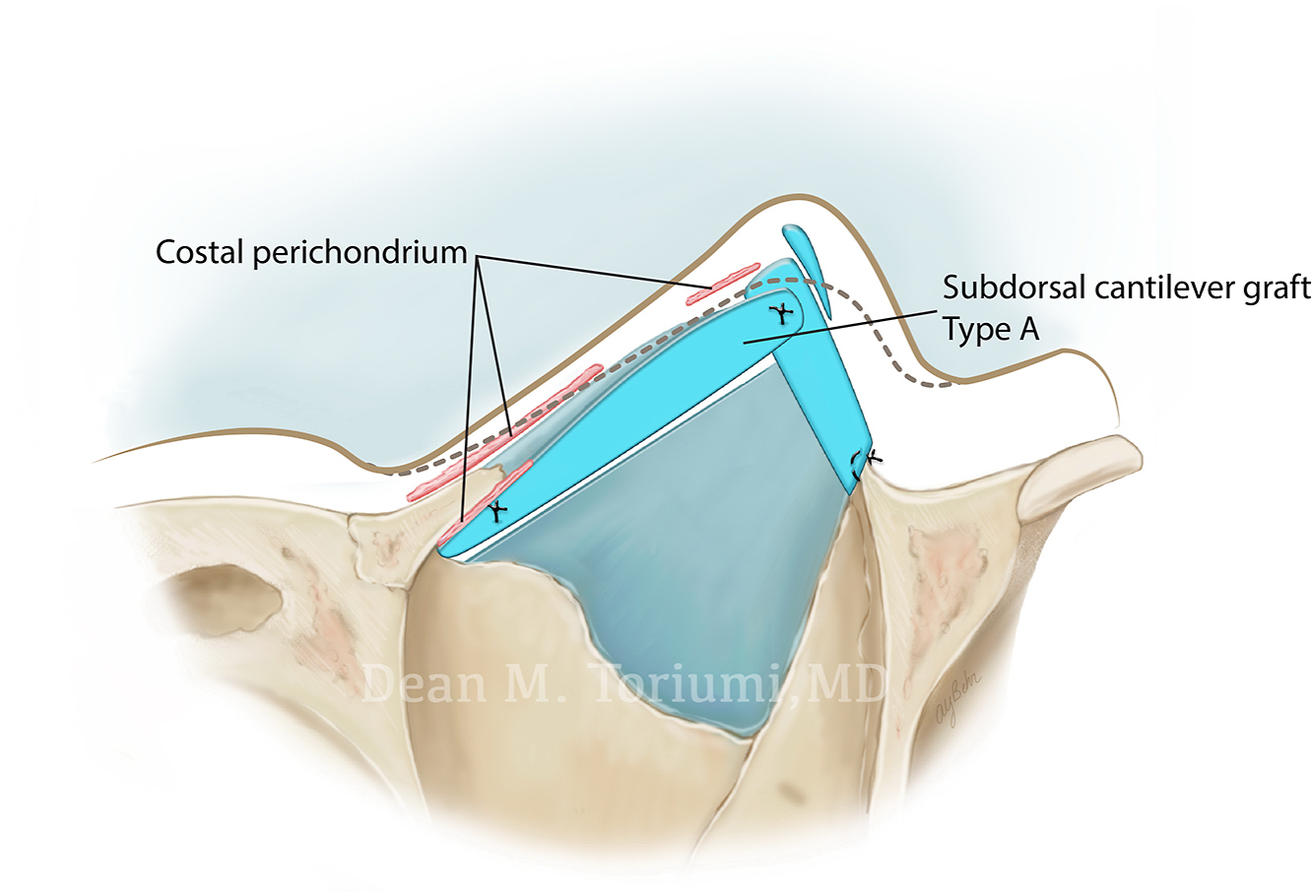
The SDCG-A is specially designed with a narrower leading edge to ensure the dorsum is not too wide. Frequently, a trough is created along the leading edge of the graft to accommodate the remnant septal keel on the undersurface of the middle vault ( Fig. 5 ). The SDCG is advanced into a space created below the nasal bones, extends under the middle vault, and is fixed to the caudal septal extension graft. With the SDCG-A, the radix is not raised, and the maximal elevation is in the middle vault.

The subdorsal cantilever graft type B (SDCG-B), is primarily used for major dorsal augmentation with radix augmentation. This would entail increases in dorsal height of 3 mm to 5 mm. After completing the subdorsal release of the septum and circumferential osteotomies, the nasal dorsum can be elevated. The bone cuts include a radix bone cut made at the level of the medial canthus, bilateral lateral osteotomies along the ascending process of the maxilla, and bilateral internal transverse bone cuts ( [CR] ). A wide subperiosteal dissection is performed along the ascending process of the maxilla to allow the nasal bones to elevate.
At this point, the SDCG can be used to raise the radix and hold the dorsum in an elevated position. To accomplish this, the cranial end of the SDCG-B graft extends through the radix bone cut to sit on top of the frontal bone and raise the radix ( Fig. 6 ). The SDCG-B is “cantilevered” off the stable frontal bone, and the bony dorsum can be reliably held in an augmented position without impacting the underlying septum. The septum can be trimmed without affecting the position of the nasal dorsum. This is why the SDCG-B can be used in reconstructive cases where there is no septal support due to injury, infection, or prior surgery.
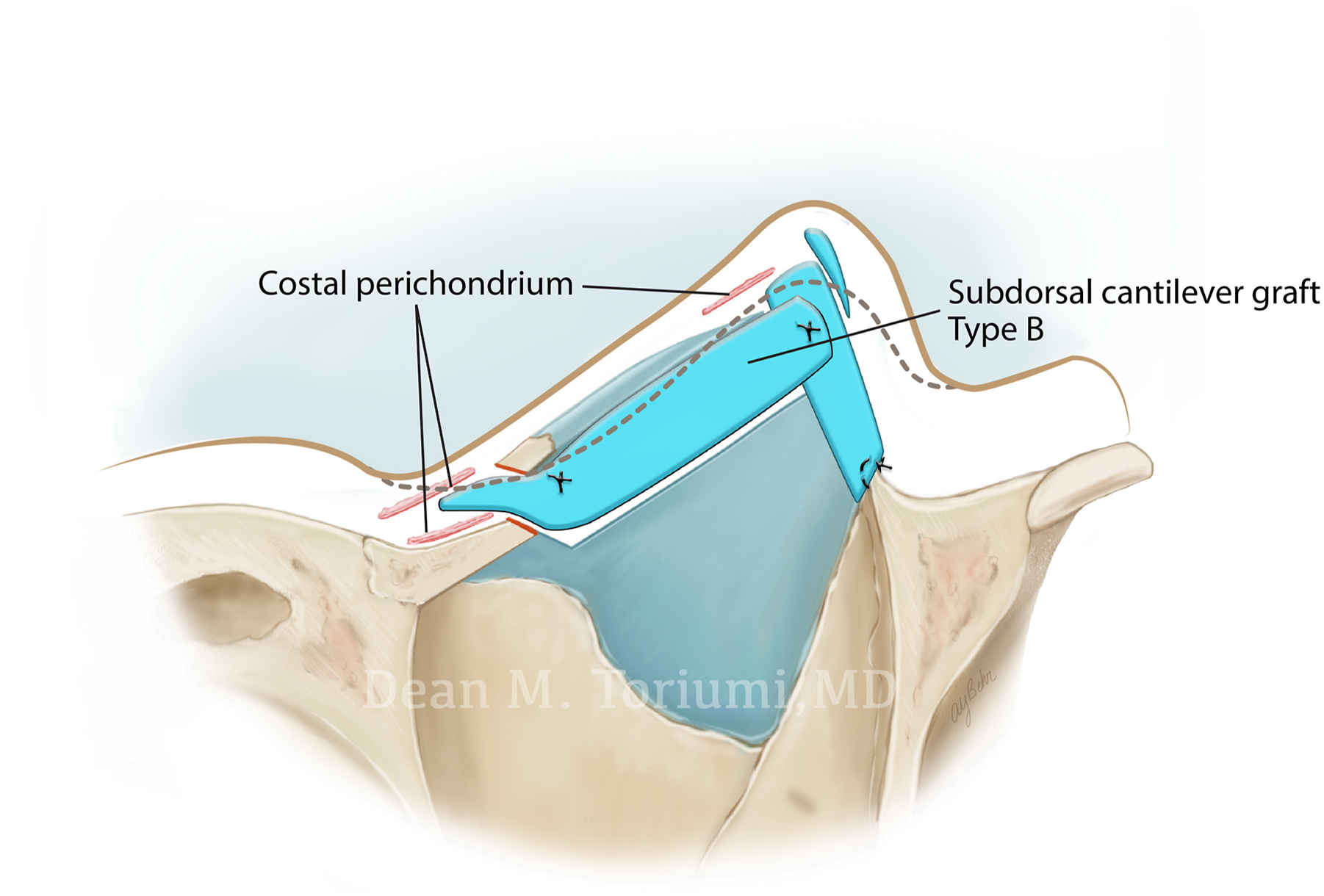
The key design feature of the SDCG-B is a distal tongue/shelf that extends through the radix bone cut with an inset to accommodate the nasal bones ( Fig. 7 ). The SDCG-B passes under the bony and middle vaults to connect to the caudal septal extension graft. The leading edge of this graft must be narrow to avoid making the dorsum too wide. Native costal perichondrium can be left on parts of the graft to aid in fixation and stabilization.

Depending on the depth of the supratip, the patient may need supratip augmentation. In such cases, the SDCG-B should have a prominence where it sits under the middle vault. This prominence under the middle vault preferentially pushes up the middle vault to accommodate the tip projection. A complete lateral keystone release and division of the piriform ligament is key to avoid tension that can result in the recurrence of the deformity. Small grafts or soft tissue grafts can be used to “fine-tune” the profile and create the final dorsal alignment.
Both the SDCG-A and SDCG-B must be very strong to raise the dorsum and middle vault and hold their positions. This is why autologous costal cartilage must be used. If the patient has softer rib cartilage, it will not support the nasal dorsum, potentially resulting in loss of dorsal augmentation. In these cases, one can harvest a costochondral graft with part bone and some cartilage. The bony portion would sit under the dorsum and the cartilage part is attached or sutured to the caudal septal extension graft. The best type of cartilage for the SDCG is partially calcified rib cartilage, as it is strong and will hold up the dorsum yet can be sutured and carved. If bone is used, a piezotome or bur can be used to sculpt the graft.
The existing septum may be in the way of the graft and may require some trimming to allow the SDCG to fit under the nasal dorsum. Additionally, the posterior edge of the graft may need to be trimmed to prevent blocking the nasal valve. The graft may create some fullness of the upper septum, but as long as it is not blocking the nasal valve it should not be a problem. Patients with a tall, narrow nose with a narrower airway are at risk for blockage of the nasal valve and may not be candidates for the SDCG. Ethnic patients requiring dorsal augmentation typically have a wider airway, more room at the nasal valve, and are less likely to experience blockage of the nasal valve.
Fixation of the graft requires drilling a transosseous hole that goes across the bony vault, allowing passage of the 4-0 polydioxanone (PDS) suture. The suture then passes through the SDCG to fix it to the nasal bones, holding the graft in place ( [CR] ). The suture will prevent the SDCG from migrating caudally and potentially losing augmentation.
At the end of the operation, the tongue of cartilage that sits on the frontal bone may need to be trimmed so there is no visible or palpable graft. Additionally, a piece of costal perichondrium or soft tissue or crushed cartilage can be placed over the radix to camouflage the cranial end of the graft. In some cases, smaller soft pieces of cartilage may be needed to fill small dorsal irregularities.
Contraindications for the Subdorsal Cantilever Graft
- 1.
Soft or weak costal cartilage. For the SDCG to be effective, the costal cartilage must be very strong and dense or even partially calcified. In some cases, a costochondral (bone and cartilage) rib graft can be used. The rib cartilage density can be assessed by using a 27-gauge needle to palpate the 7th rib. If soft or weak cartilage is used, late settling of the dorsum can result.
- 2.
Cadaver rib is not recommended for the SDCG as there is inadequate follow-up on the use of this type of cartilage for long-term structural support.
- 3.
If the surgeon is not skilled in dorsal preservation and using costal cartilage, the SDCG should not be attempted as it is a more complex technique.
- 4.
The SDCG should not be used in patients with a narrow nasal vestibule as the nasal valve could be partially blocked. Ethnic patients tend to have a wide nasal airway with room for the SDCG.
Saddle nose deformity
In the saddle nose deformity, typically there is a lack of structural support in the middle nasal vault that contributes to the saddle deformity. In some cases, there is a bony convexity with the saddling of the middle vault below. In these cases, the dorsal hump can be managed using dorsal preservation techniques, and the middle vault saddling can be pushed up from below after completely releasing the lateral keystone and the piriform ligament. The bony hump/bony cap can be rasped or reduced using an Ishida cartilaginous push down with or without bony cap preservation, or a spare roof type B. , The lateral keystone release and release of the piriform ligament are critical to the success of the SDCG, as recurrence of the deformity is possible if there is too much tension on the cartilages.
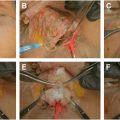
Case 1
This 32-year-old female patient presented after developing a saddle nose deformity due to trauma to her nose ( Fig. 8 ) ( [CR] ). She had nasal airway obstruction and loss of the support to her middle nasal vault. The injury occurred 5 years prior to presenting for management.
Examination revealed severe saddling of her middle vault as well as a large bony dorsal hump. Her septum was deviated as well.
This patient is a classic saddle nose deformity with a dorsal hump in the upper two-thirds of the nose and a concave “saddled” middle third of the nose. Her septum was deviated as well.
To manage her problem, I used the piezotome to perform rhinosculpture to take down her bony hump and narrow her bones. In these cases, I will avoid performing osteotomies to narrow the bones as the bony vault is the only stable structure available to act as a foundation for the reconstruction. I harvested costal cartilage due to loss of septal support and no available septal cartilage for grafting. I performed a lateral keystone release and divided the piriform ligament to allow the middle vault to push up. I also released the septum from the middle vault by performing a high subdorsal cut and also took out some bone under the bony vault using a narrow Rongeur.
To reestablish caudal septal support, I carved a caudal septal replacement graft and fixed it into a notch I made in the nasal spine (see Fig. 8 A, B).
I carved an SDCG-A with a notch caudally so it can be firmly fixed to the caudal septal replacement graft (see Fig. 8 C, D). I positioned the SDCG-A under the middle nasal vault and fixed it to a caudal septal replacement graft ( [CR] ).
I also released the lateral crura and placed costal cartilage lateral crural strut grafts to manage the nasal tip and to support the lateral wall of her nose (see Fig. 8 E, F).
The patient has done very well with correction of her saddle nose deformity (see Fig. 8 G–J).
Key points to this case
- 1.
Saddle nose deformities frequently require management of the bony hump separately from the saddle middle vault. In this case, rhinosculpture using the piezotome worked well. A bur could be used as well. I used surface preservation techniques to manage the bone deformity.
- 2.
In this case, a shorter SDCG was needed as only the middle vault needed to be elevated. Complete release of the lateral keystone and division of the piriform ligament was important to allow anterior movement of the middle vault.
Augmentation rhinoplasty
Augmentation rhinoplasty typically involves projecting the nasal tip and augmenting the nasal dorsum. Many ethnicities could benefit from increasing nasal tip projection and augmenting the nasal dorsum. As the nasal tip is projected, the need for dorsal augmentation becomes even more important to maintain balance between the upper and lower aspects of the nose. In most ethnic rhinoplasty patients, autologous costal cartilage will be needed to perform structural grafting to allow adequate, lasting increases in tip projection and dorsal augmentation.
When performing dorsal augmentation, there are many options. Many of the methods used have significant drawbacks, including graft visibility, irregularities, and resorption over time. For these reasons, the use of a SDCG can have great advantages as there are no large dorsal grafts placed on top of the dorsum, shifting and visibility are unlikely over time, and natural features of the dorsum are modified yet preserved. Since the nasal bones and middle vault are “pushed up”, the nasal bones are upper lateral cartilages provide the shape to the dorsum.
Asian augmentation rhinoplasty
Asian patients typically have a low dorsum and low radix with deficient nasal tip projection. A nuance to their management involves the changes made in the radix area. Some Asian patients do not want their radix elevated or changed. This is an important feature that needs to be discussed preoperatively in front of the computer imager so the surgeon is clear on the patient’s desires. If the patient would like the dorsum elevated to accommodate the increases in tip projection but not elevate the radix (or slight elevation of the radix), an SDCG-A is most appropriate. If the patient would like the radix elevated beyond 2 mm, then the SDCG-B is ideal and can provide up to 5 mm of radix elevation. One of the key issues here is a natural transition from the glabella to the radix and then to the dorsum. The SDCG-B can provide this natural transition, which is difficult to create with the single solid dorsal onlay graft or diced cartilage fascia graft.
Case 2
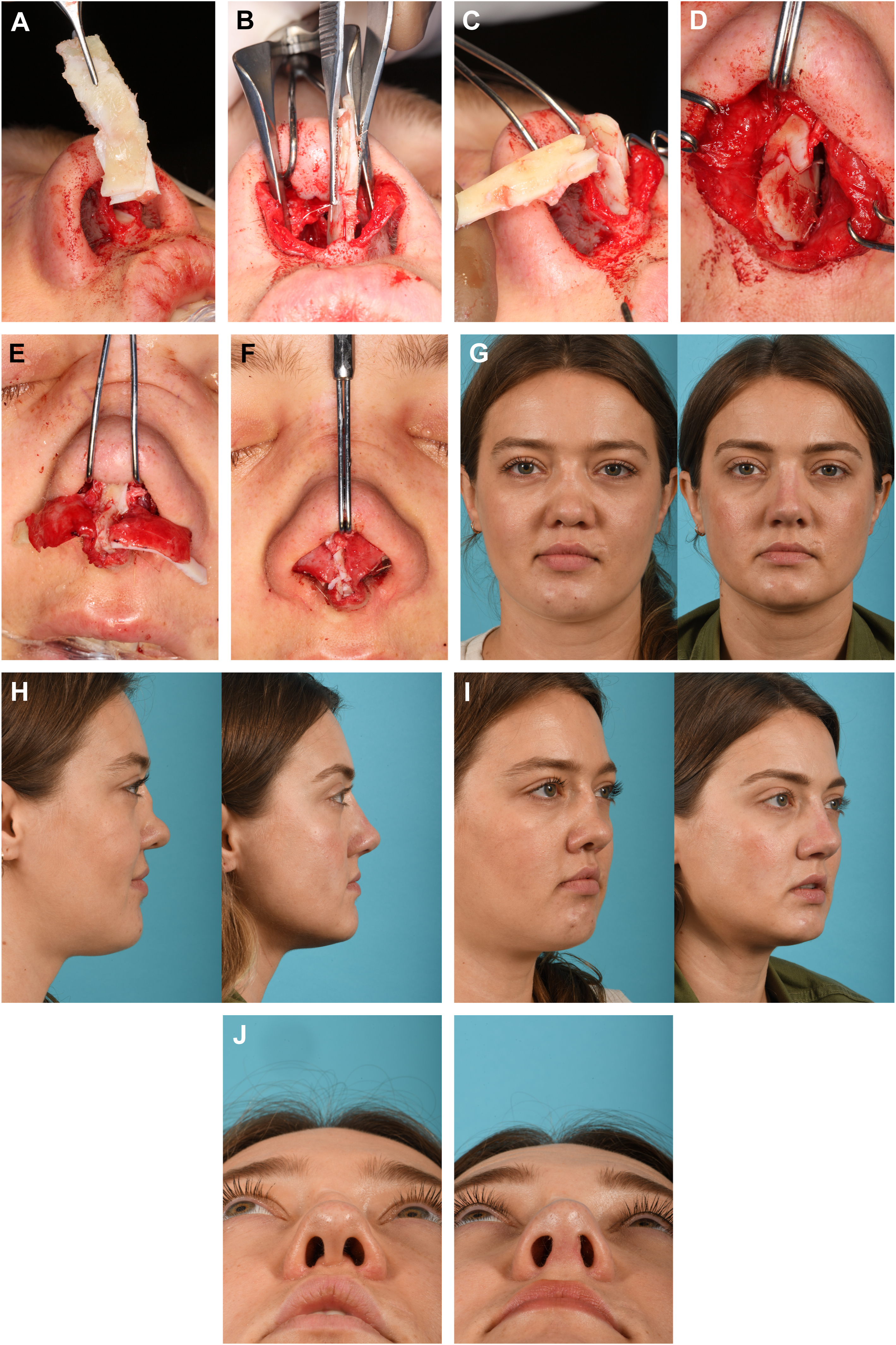
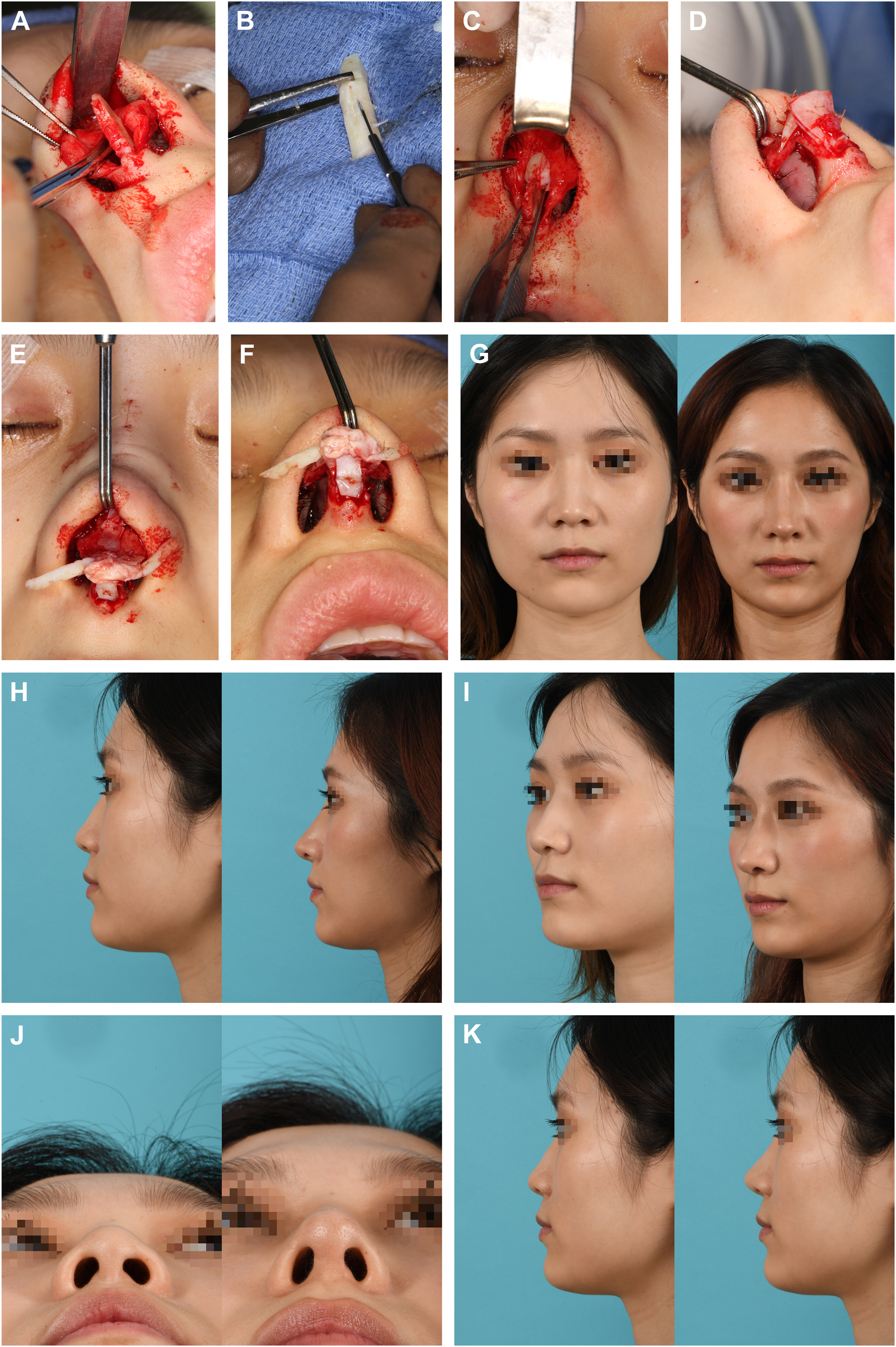
This 34-year-old Asian patient presented requesting increased nasal tip projection and augmentation of the dorsum with minimal changes to her radix position ( Fig. 9 ) ( [CR] ). She wanted only 1 mm to 2 mm of radix elevation and significant increases in tip projection.
Related posts:
 Alar Preservation Principles
Alar Preservation Principles
 Hybrid Dorsal Preservation Techniques
Hybrid Dorsal Preservation Techniques
 The Cottle Method and Modifications in Preservation Rhinoplasty
The Cottle Method and Modifications in Preservation Rhinoplasty
 The Fusion Sling—Revisiting the Nasal Tip Suspensory Anatomy
The Fusion Sling—Revisiting the Nasal Tip Suspensory Anatomy
 Cartilaginous Pushdown Nasal Hump Treatment
Cartilaginous Pushdown Nasal Hump Treatment
 Spare Roof Technique A and B – A Step-by-step Guide to Avoid Suboptimal Outcomes
Spare Roof Technique A and B – A Step-by-step Guide to Avoid Suboptimal Outcomes
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


