Human skin wounds heal largely by reparative wound healing rather than regenerative wound healing. Human skin wounds heal with scarring and without pilosebaceous units or other appendages. Dermal fibroblasts come from 2 distinct lineages of cells that have distinct cell markers and, more importantly, distinct functional abilities. Human skin wound healing largely involves the dermal fibroblast lineage from the reticular dermis and not the papillary dermis. If scientists could find a way to stimulate the dermal fibroblast lineages from the papillary dermis in early wound healing, perhaps human skin wounds could heal without scarring and with skin appendages.
Key points
- •
Human skin wounds heal largely by reparative wound healing rather than regenerative wound healing.
- •
Human skin wounds heal with scarring and without pilosebaceous units or other appendages.
- •
Dermal fibroblasts come from 2 distinct lineages of cells, one lineage populates the papillary dermis and the other lineage populates the reticular dermis, that have distinct cell markers and, more importantly, distinct functional abilities.
- •
Human skin wound healing largely involves the dermal fibroblast lineage from the reticular dermis and not the papillary dermis.
- •
If scientists could find a way to stimulate the dermal fibroblast lineages from the papillary dermis in early wound healing, perhaps human skin wounds could heal without scarring and with skin appendages.
| BLIMP | B-lymphocyte-induced maturation protein |
| CD26 | Cluster differentiation 26 (also known as DPP4) |
| DEB | Dystrophic epidermolysis bullosa |
| DLK1 | Delta-like homologue 1 |
| ECM | Extracellular matrix |
| Hsp90α | Heat shock protein 90 alpha |
| Lrig1 | Leucine-rich repeats and immunoglobulin like domains protein 1 |
| PDGFR-α | Platelet-derived growth factor receptor alpha |
| Sca-1 | (Also known as Ly6a) stem cells antigen – 1 |
Introduction
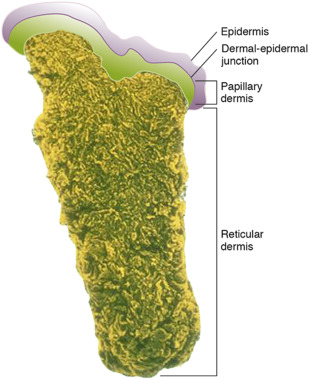
The skin is visible and readily accessible to the patient and physicians. Since the beginning of humanity, humans have manipulated their skin for medical reasons and cosmetic purposes. It has long been recognized that when surgical intervention of the skin occurs and wounding ensues at a certain depth that the skin heals with an expected scar that lacks hair and other skin appendages. Even naturally occurring diseases appear to respect a similar biological rule. The autoimmune bullous disease, pemphigus vulgaris, has an intraepidermal blister that tends to heal without scarring. In contrast, another bullous disease, dystrophic epidermolysis bullosa (DEB), features a deeper blister cleavage plane beneath the epidermal-dermal junction (specifically below the lamina densa area of the basement membrane zone), and these blisters, unlike pemphigus blister, uniformly heal with exuberant scarring. When we are talking literally about a few nanometers difference of skin depth in this direction or that direction, why is the advent of scarring or no scarring so incredibly predictable? It appears to be due to a unique lineage of fibroblasts that inhabit the papillary dermis.
The average dermatologist does between 750 and 1000 skin biopsies per year. Many of these biopsies are taken with a punch biopsy tool that ranges in size from 2 mm to 15 mm in diameter. The usual “punch biopsy” for diagnosis is usually 2 to 4 mm in size. This type of biopsy goes down through the epidermis and dermis into the subcutaneous fat, hypodermis. Fig. 1 shows the histology of such a biopsy specimen. The outer epidermal layer consists largely of epidermal keratinocytes. Interspersed within the epidermis, there are other nonkeratinocyte cells with special functions. Interspersed within the basal layer of keratinocytes there are dendritic melanocytes that make melanin and eumelanin that imparts color to the skin. Within the midepidermis there are other dendritic cells called Langerhans cells that sense invading antigens in the skin and are outposts for mounting an immune response. They are professional antigen-presenting cells and process external antigens and present them to the immune system. Last, in the epidermis there are Merkel cells, which are in association with unmyelinated free nerve endings and function to impart tactile sensory perception and light touch discrimination to the skin. The epidermis is relatively thin (0.04 mm on the eyelids), 1.6 mm, depending on the location (1.6 mm on the palms of a young adult). The average thickness of the epidermis is 0.1 mm. Nevertheless, regardless of what location of the body is examined, the dermis overall is 15 to 40 times thicker than the epidermis, depending on the anatomic site. Although the dermis may contain variable numbers of mast cells, lymphocytes, dendritic cells, and vascular endothelial cells, the main “work horse” cell for the dermis is the dermal fibroblast, spindle-shaped mesenchymal cells, which make all of the dermal components and also have the machinery to modulate and turn over dermal extracellular matrix components (ECMs). During early wound healing, the skin needs to reconstitute itself. The rent in the skin is initially filled with a fibrin clot containing fibrin, fibrinogen, fibronectin, and fragments of collagen. To resurface the wound and make an underlying vascular neodermis, 3 processes must occur: reepithelialization, fibroplasia, and neovascularization. These 3 processes require the migration of 3 critical skin cells. Keratinocytes at the cut edges of the wound need to reprogram themselves and, rather than differentiate into a stratified squamous epithelium and Stratum corneum, must become motile cells and laterally migrate across the wound bed, the process of “reepithelialization.” The clot in the wound is the initial wound bed and must transform into a neodermis. This requires the migration of periwound fibroblasts into the clot to begin laying down new collagen and other ECMs of the neodermis, the process of “fibroplasia.” The neodermis must reestablish its blood supply and this requires the ingress of periwound microvascular endothelial cells into the clot to establish new vascular tubes in the neodermis. To repair a skin wound, these 3 cells must all migrate and this migration requires an orchestration that likely involves epidermal-mesenchymal cell interactions.
Introduction
The skin is visible and readily accessible to the patient and physicians. Since the beginning of humanity, humans have manipulated their skin for medical reasons and cosmetic purposes. It has long been recognized that when surgical intervention of the skin occurs and wounding ensues at a certain depth that the skin heals with an expected scar that lacks hair and other skin appendages. Even naturally occurring diseases appear to respect a similar biological rule. The autoimmune bullous disease, pemphigus vulgaris, has an intraepidermal blister that tends to heal without scarring. In contrast, another bullous disease, dystrophic epidermolysis bullosa (DEB), features a deeper blister cleavage plane beneath the epidermal-dermal junction (specifically below the lamina densa area of the basement membrane zone), and these blisters, unlike pemphigus blister, uniformly heal with exuberant scarring. When we are talking literally about a few nanometers difference of skin depth in this direction or that direction, why is the advent of scarring or no scarring so incredibly predictable? It appears to be due to a unique lineage of fibroblasts that inhabit the papillary dermis.
The average dermatologist does between 750 and 1000 skin biopsies per year. Many of these biopsies are taken with a punch biopsy tool that ranges in size from 2 mm to 15 mm in diameter. The usual “punch biopsy” for diagnosis is usually 2 to 4 mm in size. This type of biopsy goes down through the epidermis and dermis into the subcutaneous fat, hypodermis. Fig. 1 shows the histology of such a biopsy specimen. The outer epidermal layer consists largely of epidermal keratinocytes. Interspersed within the epidermis, there are other nonkeratinocyte cells with special functions. Interspersed within the basal layer of keratinocytes there are dendritic melanocytes that make melanin and eumelanin that imparts color to the skin. Within the midepidermis there are other dendritic cells called Langerhans cells that sense invading antigens in the skin and are outposts for mounting an immune response. They are professional antigen-presenting cells and process external antigens and present them to the immune system. Last, in the epidermis there are Merkel cells, which are in association with unmyelinated free nerve endings and function to impart tactile sensory perception and light touch discrimination to the skin. The epidermis is relatively thin (0.04 mm on the eyelids), 1.6 mm, depending on the location (1.6 mm on the palms of a young adult). The average thickness of the epidermis is 0.1 mm. Nevertheless, regardless of what location of the body is examined, the dermis overall is 15 to 40 times thicker than the epidermis, depending on the anatomic site. Although the dermis may contain variable numbers of mast cells, lymphocytes, dendritic cells, and vascular endothelial cells, the main “work horse” cell for the dermis is the dermal fibroblast, spindle-shaped mesenchymal cells, which make all of the dermal components and also have the machinery to modulate and turn over dermal extracellular matrix components (ECMs). During early wound healing, the skin needs to reconstitute itself. The rent in the skin is initially filled with a fibrin clot containing fibrin, fibrinogen, fibronectin, and fragments of collagen. To resurface the wound and make an underlying vascular neodermis, 3 processes must occur: reepithelialization, fibroplasia, and neovascularization. These 3 processes require the migration of 3 critical skin cells. Keratinocytes at the cut edges of the wound need to reprogram themselves and, rather than differentiate into a stratified squamous epithelium and Stratum corneum, must become motile cells and laterally migrate across the wound bed, the process of “reepithelialization.” The clot in the wound is the initial wound bed and must transform into a neodermis. This requires the migration of periwound fibroblasts into the clot to begin laying down new collagen and other ECMs of the neodermis, the process of “fibroplasia.” The neodermis must reestablish its blood supply and this requires the ingress of periwound microvascular endothelial cells into the clot to establish new vascular tubes in the neodermis. To repair a skin wound, these 3 cells must all migrate and this migration requires an orchestration that likely involves epidermal-mesenchymal cell interactions.
Related posts:
 Basic Science Insights into Clinical Puzzles
Basic Science Insights into Clinical Puzzles
 Establishing Tolerance to Commensal Skin Bacteria
Establishing Tolerance to Commensal Skin Bacteria
 Dermatologic Manifestations of Monogenic Autoinflammatory Diseases
Understanding Inherited Cylindromas
Dermatologic Manifestations of Monogenic Autoinflammatory Diseases
Understanding Inherited Cylindromas
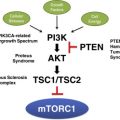 Mosaic Disorders of the PI3K/PTEN/AKT/TSC/mTORC1 Signaling Pathway
Interleukin-22 and Cyclosporine in Aggressive Cutaneous Squamous Cell Carcinoma
Mosaic Disorders of the PI3K/PTEN/AKT/TSC/mTORC1 Signaling Pathway
Interleukin-22 and Cyclosporine in Aggressive Cutaneous Squamous Cell Carcinoma
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


