This article presents the diagnosis and treatment of distal radius fractures with emphasis on (1) current common principles, (2) the author’s current practices, and (3) controversies. The author emphasizes that displaced distal radius fractures should be approached first with a trial of closed reduction, with or without percutaneous pinning. If this reduction is unstable or unsuccessful, open reduction is indicated. Early treatments include percutaneous pinning through the distal radioulnar joint, early or delayed reattachment/repair of the avulsed dorsal periphery of the triangular fibrocartilage complex (TFCC), reattachment of the TFCC to the ulna fovea, and late reconstruction.
Key points
- •
Displaced distal radius fractures are attempted first by closed reduction (sometimes multiple attempts), with or without percutaneous pinning. Open reduction is indicated if reduction is unstable or unsuccessful with resultant dorsal angulation of more than 20°, step-off in the articular surface of more than 1 mm, or radial shortening of more than 3 to 5 mm.
- •
More conservative methods should be used when treating elderly patients. Dorsal angulation of 20° to 30° in the elderly is not a strict indication for open repair.
- •
Ulnar-side ligament injury is a major concern in distal radius fractures. Early treatments include percutaneous pinning through the distal radioulnar joint, early or delayed reattachment/repair of the avulsed dorsal periphery of the triangular fibrocartilage complex (TFCC), reattachment of the TFCC to the ulna fovea, and late reconstruction.
- •
This article presents the diagnosis and treatment of distal radius fractures with emphasis on (1) current common principles, (2) the author’s current practices, and (3) controversies.
A great amount of discussion has been directed toward distal radius fracture. This review is not intended to recite recent innovations or summarize well-known, classic literature for the readers. Rather, information is presented that was learned in the author’s practice and from the author’s colleagues through their cases and publications; the author focuses on diagnostic tools, treatment selection, and current controversial issues.
Volume of practice
Over the past 10 years, in the author’s unit alone, they treat a steady number (ranging from 300 to 350) of distal radius fractures annually. Simply because of China’s population, hand surgeons in China see among the largest numbers of distal radius fractures treated in the world. These fractures are, thus, among the most often discussed in Chinese literature, though few of these reports have been made in English.
It was impossible to follow all 3500 patients treated either operatively or nonoperatively over the 10-year period by the 12 hand surgeons in the author’s unit. Consequently, the author selectively followed a few patient groups on their outcomes following various treatment techniques.
Incidence
Author’s team members (Dr Guheng Wang and others) looked at distal radius fractures in summer and winter seasons based on electronic records of the hospital. From May to August 2008, 1395 fractures (669 upper extremity fractures) were treated, among which 105 were distal radius fractures (31 of which were accompanied with ulnar styloid fractures). From December 2008 to February 2009, 79 distal radius fractures were treated (among which 28 were accompanied with ulnar styloid fractures). The monthly incidences of distal radius fractures in the summer and in the winter were similar. The author’s city is located at the costal line where the Yangtze River enters the Pacific Ocean with distinct hot and cold seasons with occasional snowfalls and plentiful outdoor activities in the winter. The accompanied ulnar styloid fracture was seen in 31% (27% in the summer and 35% in the winter) of the patients.
Distal radius fractures accounted for 7.5% of all fractures and for 15.7% of all upper extremity fractures, second only to the 30% incidence of phalangeal fractures according to our data in 2008.
Incidence
Author’s team members (Dr Guheng Wang and others) looked at distal radius fractures in summer and winter seasons based on electronic records of the hospital. From May to August 2008, 1395 fractures (669 upper extremity fractures) were treated, among which 105 were distal radius fractures (31 of which were accompanied with ulnar styloid fractures). From December 2008 to February 2009, 79 distal radius fractures were treated (among which 28 were accompanied with ulnar styloid fractures). The monthly incidences of distal radius fractures in the summer and in the winter were similar. The author’s city is located at the costal line where the Yangtze River enters the Pacific Ocean with distinct hot and cold seasons with occasional snowfalls and plentiful outdoor activities in the winter. The accompanied ulnar styloid fracture was seen in 31% (27% in the summer and 35% in the winter) of the patients.
Distal radius fractures accounted for 7.5% of all fractures and for 15.7% of all upper extremity fractures, second only to the 30% incidence of phalangeal fractures according to our data in 2008.
How does the author handle these patients?
Diagnosis
On arrival, anteroposterior, lateral, and oblique radiograph views are routinely taken. Plain films are instrumental in making the diagnosis. Although deformity of the distal radius can be very obvious, nondisplaced fractures may be subtle to detect during the physical examination, sometimes presenting as pain and point tenderness without obvious swelling or deformity.
Few controversies exist regarding the methods of nonoperative treatment; however, opinions on indications for nonoperative management vary among surgeons. There is a trend toward overtreating this fracture surgically in many units. The author stresses that surgeons should amply consider the option of closed reduction before proceeding with less conservative treatments.
Indications of Treatment
The key practice guidelines for treating distal radius fractures:
Absolute indications for conservative treatment
- 1.
Incomplete fracture
- 2.
Nondisplaced complete fracture
- 3.
Displaced extra-articular fracture, which can be reduced to a stable fracture with acceptable deformity*
- 4.
Other injuries/conditions (too elderly or severely traumatized) that are a contraindication to surgery
∗ Surgical Notes: Acceptable deformity is defined as less than 2 mm of radial shortening, less than 10 degrees of dorsal angulation of the distal articular surface, and 0 mm in joint incongruity after manual reduction of the fracture (simply remembered as 2-1-0).
Relative indications for conservative treatment
- 1.
Displaced extra-articular fracture, which can be reduced to 10° to 20° of dorsal angulation, with a reduction that is likely unstable
- 2.
Shortening of the distal radius just more than 2 mm
- 3.
Comminuted extra-articular fracture with a small extra-articular fragment left unreduced after closed reduction, with 2 larger distal and proximal fragments that are reduced and stable
- 4.
Dorsal angulation of more than 20° in the elderly
Indications for closed reduction and percutaneous pinning
- 1.
All of the 4 aforementioned relative indications for conservative treatment can be treated with closed reduction and percutaneous pinning (CRPP) (or other minimally invasive methods, such as segment-specific fixation).
- 2.
Displaced, unstable intraarticular fractures in which the displaced distal fragment is large, amenable to being fixed percutaneously
- 3.
CRPP helps preserve the reduction in an extra-articular fracture that is unstable after reduction.
- 4.
Displaced radial styloid fracture
Indications for open reduction and internal fixation
- 1.
Intraarticular fractures whose reduction does not restore a congruent articular surface (ie, a step-off >1 mm), especially when multiple fragments are present∗∗
- 2.
Extra-articular fracture is comminuted with reduction that is unsuccessful or unstable
- 3.
Radial shortening of more than 5 to 10 mm, which cannot be reduced and stable without an open approach
- 4.
Open wound with significant soft tissue loss
- 5.
Accompanied by an ulnar shaft fracture
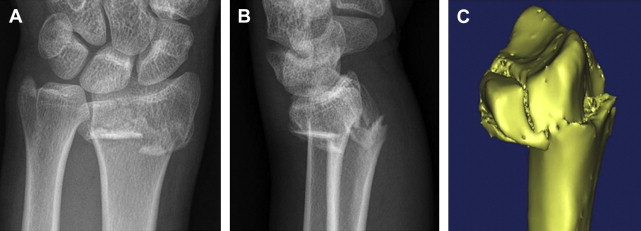
∗∗ Surgical Notes: These groups of patients are best assessed with a computerized tomography (CT) scan and 3-dimensional (3D) images to evaluate joint step-offs, distal radioulnar joint (DRUJ) involvement, and direction of displacement of multiple fragments ( Fig. 1 ).
The aforementioned indications provide a quick reference for surgeons, from experienced to trainees, in emergency settings in the author’s unit and reflect their practice guidelines. AO classification is determined and treatment selected in the making of the diagnosis, evaluation of images, and discussed among the surgical team. Three-dimensional image reconstruction is used for accurately locating fracture fragments (see Fig. 1 ).
Concomitant injuries are common
DRUJ Instability or Subluxation
The DRUJ structures are often injured in wrist trauma and should be treated either at the time that the fractures are addressed or soon after fracture healing. Any displaced distal radius fracture affects the DRUJ; mild disturbance to the ligaments (including elongation or partial tear) heal without surgical treatment when a distal radius fracture is reduced. DRUJ instability should only be specifically attended at the time of distal radius fracture if there are signs of instability or subluxation. Tenderness and pain over the DRUJ are not sufficient to make the diagnosis. When radiological evidence of apparent joint widening or physical signs of relative motion of the ulna from the radius (piano key sign) ( Fig. 2 ), the diagnosis is established and treatment is warranted.
Ulnar Styloid Fracture Through Tip, Body, or Base
Ulnar styloid fractures are seen in 33% of distal radius fractures in the author’s data set. The author does not specifically treat these fractures, even if they are displaced.
Carpal Ligament Injury and Triangular Fibrocartilage Complex Injury
Carpal ligament injuries are very prevalent and, with the exception of Geissler grade III and IV injuries, which account for less than 10% of ligamentous injuries, most do not need surgical repair. Triangular fibrocartilage complex (TFCC) injuries should be treated when there is avulsion of either the dorsal peripheral attachment or of the insertion on the ulnar styloid or fovea.
Fractures in the Carpal Bones, Metacarpus, or Phalanges
According to the author’s data, 0.26% of distal radius fractures are accompanied with carpal bone fractures, 0.79% with metacarpal fractures, and 0.33% with phalangeal fractures. These fractures are treated independently.
Next, conservative management and each common surgical treatment of distal radius fractures and their concomitant injuries are outlined.
Conservative treatment
Nonsurgical treatment is based around using a full forearm cast for complete fractures or a dorsal splint in incomplete fractures. The cast is shaped with the wrist in a functional position for the carpus. If the fracture has dorsal angulation before reduction, the wrist is kept in moderate flexion with ulnar deviation ( Fig. 3 ). The author applies a below-elbow cast, with the forearm slightly supinated or in neutral rotation, extending distally to the level of the thumb and finger metacarpophalangeal (MCP) joints; this cast allows full range of digital motion at the MCP joints. The cast is removed after 5 to 7 weeks when the bone healing is confirmed on plain radiographs. The duration of healing can vary. An incomplete fracture heals in 4 to 5 weeks; a reduced complete fracture needs 5 to 6 weeks; elderly patients typically require 6 or more weeks regardless of the fracture severity.
Under anesthesia, sufficient traction is the first step for a proper reduction. The mini-C arm machine is useful for confirming reduction. The reduced fracture can be pinned if repeat reductions fail to maintain stable alignment or to correct dorsal tilt, radial deviation, or radial shortening.
Surgical treatment
CRPP
CRPP is the immediate next step for fractures that fail to achieve stable, maintained, adequate reduction. One or 2 Kirschner wires (K-wires) (0.045–0.056 in) maintain the reduction in most fractures ( Fig. 4 ), but a large fragment may need more than 2 K-wires. If more than 2 fragments exist, 3 or more K-wires are used. For a simple radial styloid fracture, one pin is adequate. For all of the aforementioned fractures, the K-wires are inserted most often from the radial styloid or from the dorsolateral cortex of the radius under the guidance of a mini-C arm. With the image intensifier, the K-wires should be confirmed to cross the fracture line and extend to the opposite cortex.
One or 2 cannulated screws can be used instead of K-wires; these are particularly useful for repairing radial styloid fractures because they provide compression at the reduction.
Open Reduction and Internal Fixation
Plate fixation
This tool is a major tool for internal fixation. The plate system is evolving continually. A volar approach is always favored in the author’s unit.
- 1.
Skin incision of 8 to 10 cm is made between the flexor carpi radialis (FCR) tendon and the radial artery. Care is taken to preserve branches of the median nerve, which are ulnar to the FCR tendon ( Figs. 5 and 6 ).
Fig. 5
( A ) The plates of different sizes and lengths are available. ( B ) Placement of compression locking screws.
Fig. 6
The locking compression plates (Synthes Inc) for comminuted intraarticular fracture of the distal radius. ( A , B ) Preoperative plain radiographs. ( C ) Surgical incision and exposure of the FCR tendon. The access is made radial to the FCR tendon. ( D ) After fracture reduction and placement of the plate. ( E , F ) Postoperative radiographs showing reduction of the joint surface and fracture.
( From Tang JB, editor. Distal radius fracture. Shanghai (China): Shanghai Science and Technology Press; 2013. p. 155–6; with permission; and Courtesy of Synthes, Inc, West Chester, PA, with permission.)
- 2.
The FCR tendon is retracted ulnarly, and the radial vascular bundle is retracted radially.
- 3.
The pronator is elevated as an ulnarly based flap by dividing its insertion on the radius.
- 4.
The fracture is reduced, and the plate is placed. Before plating, K-wires can be used to temporarily hold the fracture fragments in reduction; surgical clamps can also be used for this purpose.
- 5.
The plate is fixed by inserting screws that lock into the threaded holes in the distal plate. The plate is then fixed proximally using self-tapping screws (see Fig. 6 ).
- 6.
The implant is then covered with the pronator quadratus, which is sutured back in its appropriate place. If the insertion of the brachioradialis is split, the split portion of the brachioradialis tendon is also sutured back. The skin is closed. A light splint is applied for 5 weeks, and active wrist motion begins by week 2 or 3.
Surgical Points: ( 1 ) Do not project the plate distally over the watershed line or it can irritate the flexor tendons. ( 2 ) Low-profile plates are desirable. ( 3 ) K-wires can supplement fracture fragment reduction when a plate does not suffice. ( 4 ) The screw length should be 1 or 2 mm shorter than the depth gauge readings to prevent screw-tip injury to the extensor tendons.
The volar approach is a popular method, which is particularly useful if the volar fragment is large and displaced ( Fig. 7 ). The dorsal plate is only occasionally used, with a different plate design ( Fig. 8 ). Extensor tendons should be protected and should not contact the dorsally placed plate.
Many plating systems are developed and available from a variety of companies. The surgeon should decide which plates and methods to use. In the author’ follow-up data, newer-generation plates have not shown statistically better functional outcomes compared with earlier models. Newer plates are often easier to insert and achieve reduction.
Segment-specific fixation
This method has gained popularity and is a future direction for open reduction and fixation. The surgery is done through a minimally invasive approach, and achieved fixation is efficient and stable. Postoperative early active motion is allowed if the fracture involves a single column of the wrist. This method is most appropriate for fracture fragments not amenable to stable fixation without open repair, with fragments too small for the use of ordinary plates ( Fig. 9 ).
External fixator
The author uses an external fixator when a soft tissue defect is large and contaminated or when the articular surface is significantly compressed with multiple bursting fragments ( Fig. 10 ). This fixation should be applied within 2 weeks of the injury, otherwise tissue healing makes adequate reduction difficult. Internal fixation is usually necessary simultaneously, but it can be added days later once local wound conditions have improved. To restore joint surface congruency or to fix multiple fragments, multiple methods of fixation (external fixation, multiple pins or plates, or segment-specific devices) can be used together. An external fixator restores forearm length, but it alone cannot restore stable joint surface anatomy.







