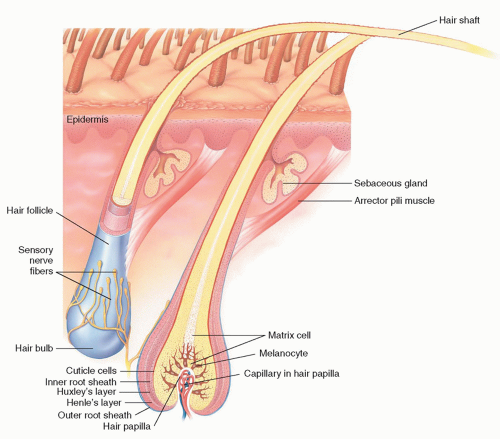
 FIG. 14-1. Anatomy of hair. |
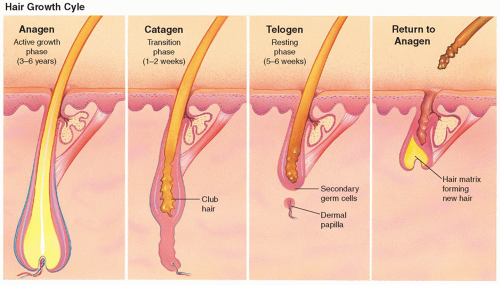 FIG. 14-2. Hair growth cycle. |
TABLE 14-1 Characteristics of Alopecia for Differential Diagnosis | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||
Alopecia areata (diffuse)
Telogen or anagen effluvium
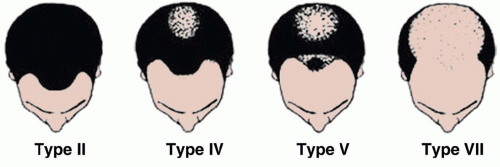 FIG. 14-3. Hamilton-Norward classification of male pattern baldness. |
TABLE 14-2 Evaluation of Hair Loss: History | ||||||
|---|---|---|---|---|---|---|
|
Location and pattern of hair loss
Diffuse or localized
Complete loss or thinning
Hair texture, length, and color
Presence of scarring
Presence of erythema, pustules, scale, or abnormal pigmentation
Nail findings
Acne or hirsutism
Patient affect and behaviors (i.e., anxiety)
Not often necessary but are guided by specific differential diagnoses.
Fungal cultures can help to confirm tinea.
Serologies help identify underlying disease causing alopecia: complete blood count and ferritin (iron-deficiency anemia); RPR (syphilis); antinuclear antibodies (autoimmune diseases); and TSH, T4, and thyroid antibodies (hypothyroidism).
In women, serum testosterone (free and total), DHEAS, and prolactin levels (if galactorrhea is present).
Additional hormonal studies should be done in the presence of menstrual irregularities or hormonal abnormalities.
Telogen effluvium (acute and chronic)
Diffuse alopecia areata
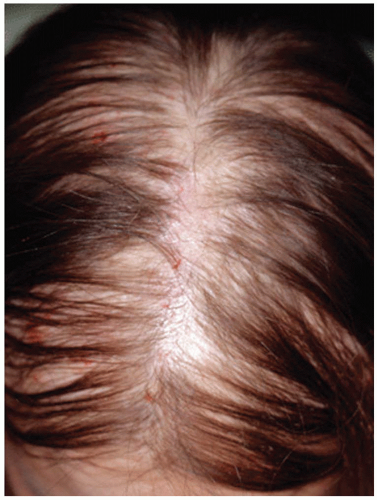 FIG. 14-4. Female pattern hair loss begins with widening central part and diffuse thinning. |
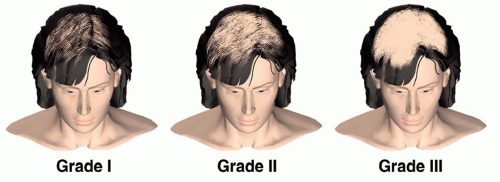 FIG. 14-5. Ludwig classification of female pattern hair loss. Note the retention of the frontal hairline despite the increasing severity of hair loss. |
Female pattern hair loss
Diffuse alopecia areata
2 weeks after the chemotherapy. After the chemotherapy or drug is discontinued, hair growth resumes. Occasionally, hair texture and color are different than pretreatment. Topical minoxidil can shorten the time of baldness by an average of 50 days, aiding in faster regrowth of hair once chemotherapy has been discontinued (Figure 14-6).
 FIG. 14-6.
Get Clinical Tree app for offline access
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|