Classification
Disease
Occupational leukoderma
Phenols and other derivatives
Genetic syndromes
Piebaldism
Tuberous sclerosis
Hypomelanosis of Ito
Malformations
Nevus anemicus
Nevus depigmentosus
Idiopathic
Idiopathic guttate hypomelanosis
Lichen sclerosus et atrophicus
Infections
Tinea versicolor
Leprosy
Syphilis
Neoplastic
Mycosis fungoides
Halo nevus
Postinflammatory hypopigmentation
Pityriasis alba
Atopic dermatitis/allergic contact dermatitis
Phototherapy-induced hypopigmentation
Hypopigmented scar
Psoriasis
Discoid lupus erythematosus
Scleroderma
Topical drug-induced depigmentation
24.2 Genetic Syndromes
24.2.1 Piebaldism
Piebaldism is an autosomal dominant disorder in tyrosine kinase transmembrane receptor of the melanocyte. This congenital condition is characterized by an extensive, symmetrically distributed depigmented areas. It has been reported in all races with equal sex distribution [2]. Midfrontal poliosis (Fig. 24.1) is seen in 80–90 % of cases. Depigmentation, however, may cover minimal to extensive areas of the entire body. Histopathology reveals a decreased number or total absence of melanocytes and melanin.
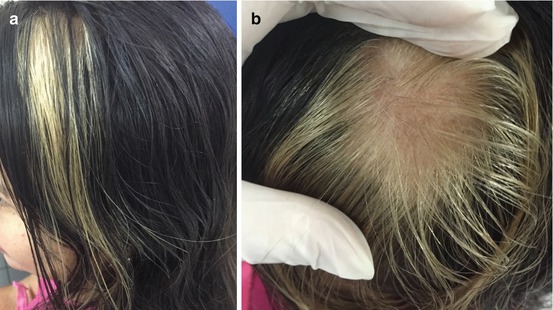
Fig. 24.1
Midfrontal poliosis in a Filipina with piebaldism
24.2.2 Tuberous Sclerosis
Tuberous sclerosis complex (TSC) is an autosomal dominant multisystem neurocutaneous syndrome with characteristic features of multiple hamartomas distributed throughout the skin, central nervous system (CNS), eye, heart, kidney, liver, and lungs. Two-thirds of cases are sporadic. The true incidence of this condition is unknown but reports were between 1 in 5,800 and 1 in 10,000 [4].
There are two different types of hypopigmented macules in TSC: medium- to large-sized hypopigmented macules and tiny confetti-like macules. The ash-leaf macule/spot, which can be mistaken for a vitiligo lesion, is the most characteristic type of hypopigmented lesion in TSC. It is lance-ovate shaped, often linear, usually 1.0–12 cm in diameter, with one end rounded and the other sharp tipped (Fig. 24.2). This typical lesion predilects the trunk and buttocks.
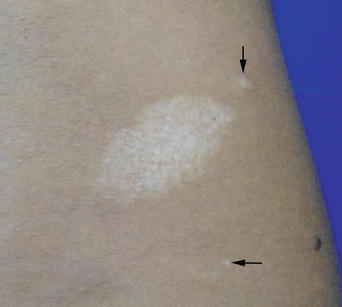
Fig. 24.2
Hypomelanotic patch in TSC: notice the large ash-leaf spot and small confetti-like lesions (arrows) on the left thigh of a Filipino patient
The confetti-like lesions (Fig. 24.2, arrows) are characterized by tiny 1–3 mm white spots, symmetrically distributed, typically over the extremities. The hypopigmentation is enhanced by Wood’s lamp examination. Histopathology reveals reduction in the number of melanocytes and a decrease in melanosome size and epidermal melanin.
There are notable cutaneous findings in TSC, not evident in vitiligo. Facial angiofibromas are benign hamartomas pathognomonic of TSC, which appear as multiple smooth, firm, pink, 1–5-mm papules over the nasolabial folds, cheeks, and chin (Fig. 24.3a). Shagreen patch is a connective tissue nevus appearing as skin-colored to yellow plaques with irregular pebbled surface and is typically located over the back and buttocks (Fig. 24.3b). Periungual fibromas or angiofibromas are seen as conical, pink, firm projections from the proximal nail folds of fingers and toes which usually arise during puberty.
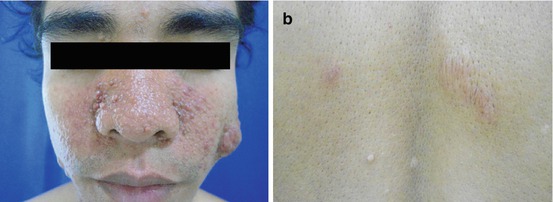
Fig. 24.3
Filipino male with facial angiofibromas on the nasolabial folds (a) and shagreen patches on the back (b)
Extracutaneous manifestations, if present in TSC, differentiate it further from vitiligo:
CNS: Tumors producing seizures such as cortical tubers, periventricular calcification, subependymal hamartomas, astrocytomas, infantile spasms, and mental retardation.
Eye: Retinal hamartomas (phakomas) are seen in 50 % of patients with tuberous sclerosis which appear as gray to yellow plaques on the retina.
Heart: Cardiac rhabdomyoma.
Kidney, liver, thyroid, testes, and GIT: Hamartomas of mixed cell type.
Others: Angiomyolipoma, multiple renal cysts, enamel pits, gingival fibromas, phalangeal cysts, periosteal thickening, and pulmonary cysts.
The management of TSC is presently symptomatic. However, some recent therapeutic trials of mammalian target of rapamycin (mTOR) pathway antagonists such as rapamycin (sirolimus) showed potential therapeutic options for TSC patients [4].
24.3 Malformations
24.3.1 Nevus Anemicus
Nevus anemicus (Fig. 24.4) usually presents at birth with an irregularly shaped hypochromic patch, varying from one to several centimeters in size. The contrast with the surrounding non-lesional skin disappears upon application of pressure [5]. Highly sensitive α-adrenergic receptors of endothelial cells in the affected areas lead to vasoconstriction of small vessels; E-selectin expression is reported to be decreased [6]. Emotional stress and physical activities are shown to be trigger factors. The lesion is usually found on the trunk but the face and extremities may be affected. No abnormal findings are noted on histopathologic evaluation, differentiating it from vitiligo. No treatment is needed for this condition.

Fig. 24.4
Nevus anemicus on the back of a 25-year-old Filipino male. Histopathology showed normal skin findings
24.3.2 Nevus Depigmentosus
Nevus depigmentosus presents as a well-circumscribed irregularly bordered hypopigmented macule or patch that becomes visible from birth or during the first year of life. It presents as hypopigmentation rather than depigmentation, in contrast to vitiligo. It remains stable in its relative size and distribution throughout life. A defect in the transfer of melanosomes from melanocytes to keratinocytes has been reported [7]. There are three clinical variants: isolated (solitary and well-defined lesion) (Fig. 24.5), segmental (unilateral, band-shaped, Blaschkoid distribution lesions), and systematized form (extensive, whorls, and streaks of hypopigmentation following the lines of Blaschko). Nevus depigmentosus is usually not associated with any systemic manifestations. However, the variants manifesting with the Blaschkoid pattern have been associated with developmental disorder and epilepsy. Histopathology reveals marked reduction of melanin with variable melanocyte count (normal to decreased).

Fig. 24.5
Nevus depigmentosus, isolated variant, present at birth in a Filipino patient
Camouflage may be required. Surgical grafting has been reported with poor to good repigmentation; recurrence was noted during follow-up [3].
24.4 Idiopathic
24.4.1 Idiopathic Guttate Hypomelanosis
Idiopathic guttate hypomelanosis (IGH) is a common, benign, idiopathic leukodermic dermatosis, which manifests as asymptomatic, small, 0.2–1.6 cm, achromic, or hypopigmented macules on the sun-exposed areas of the upper and lower extremities (Fig. 24.6). Patients usually have associated signs of photoaging, including atrophy, lentigines, and xerosis. This condition is commonly seen among the elderly, over the age of 50, with female predisposition [8].

Fig. 24.6
Idiopathic guttate hypomelanosis on the right forearm of a 65-year-old male gardener
The pathogenesis of IGH is not completely understood, but a multifactorial etiology is more likely to be involved, such as senile degeneration, sunlight exposure, and trauma. On histopathology, slight basket-weave hyperkeratosis with epidermal atrophy and flattening of the rete ridges is seen. There is a decrease in melanocytes and epidermal melanin with irregular distribution of pigment granules.
Vitiligo differs from IGH in terms of both age of onset and the size and distribution of lesions. Together with sun protection, reassurance is required in most patients with IGH. Topical tretinoin, steroids, and calcineurin inhibitors have been proposed to improve the lesions of IGH. However, careful destruction using trichloroacetic acid, liquid nitrogen, or superficial dermabrasion is the most effective treatment [9, 10]. Some reports also showed promising result with fractional CO2 laser [11].
24.5 Infections
24.5.1 Leprosy (Hansen’s Disease)
Leprosy is a chronic mycobacterial infection of the skin and peripheral nerves that is caused by Mycobacterium leprae. According to the World Health Organization (WHO), endemic countries for leprosy are India, Brazil, Indonesia, Nigeria, Ethiopia, Bangladesh, and other countries in Southeast Asia, Africa, and Western Pacific region [12]. The Ridley-Jopling classification divided the disease into tuberculoid (TT), borderline (BT, BB, BL), and lepromatous leprosy (LL). The WHO supports only two spectrums, based on the number of acid-fast bacilli (AFB) found in the tissues: paucibacillary (PB) and multibacillary (MB) leprosy. The lesions of leprosy may manifest as solitary to multiple hypopigmented patches (Fig. 24.7) with hypoesthesia and sometimes accompanied by enlargement of peripheral nerve or palsy. Histopathological examination reveals granulomatous dermal infiltrate of predominant foamy histiocytes in perivascular, periadnexal, and perineural areas with or without grenz zone. A definite diagnosis of leprosy requires demonstration of a consistent peripheral nerve abnormality or AFB in tissues. Slit-skin smear examination with modified Ziehl-Neelsen stain will help to demonstrate the AFB. Absence of hypoesthesia, nerve abnormalities, and distinct histopathology findings clearly distinguish vitiligo from leprosy.