Fig. 9.1
Postinflammatory hyperpigmented patches in an elderly Filipino female with dermatomyositis (Courtesy of the Research Institute for Tropical Medicine, Philippines)
PIH can occur at any age with no gender preference. Epidermal PIH can result from acne, insect bites, pyodermas, atopic dermatitis, psoriasis and pityriasis rosea. It generally resolves over time, although fading may require months or years in darkly pigmented individuals [2].
On the other hand, dermal PIH has been associated with dermatoses characterized by degeneration of the basal layer of the epidermis and inflammation at the dermal-epidermal junction such as lupus erythematosus and fixed drug eruptions. Resolution is slower and longer than epidermal PIH, and treatment is a challenge.
9.2 Exogenous Ochronosis
Exogenous ochronosis is an uncommon disorder characterized by dark brown to black or blue-black hue (Fig. 9.2) caused by the deposition of microscopic, ochre‑colored pigment in the dermis [3, 4].

Fig. 9.2
Dark bluish-black pigmentation on the cheeks of a Filipino female after prolonged used of hydroquinone-containing OTC products (Courtesy of the Research Institute for Tropical Medicine, Philippines)
It has been seen as a result of hydroquinone use among dark-skinned individuals. The condition, however, may also develop from the use of antimalarials and products containing resorcinol, phenol, mercury and picric acid [1]. Skin irritation and vigorous friction may be contributory as well. Histopathology is definitive, with the banana-shaped ochronotic fibers in the dermis.
9.3 Acquired Bilateral Nevus of Ota-Like Macules (ABNOM)
Acquired bilateral nevus of ota-like macules are multiple, speckled blue-brown and/or slate-gray macules occurring bilaterally on the malar regions (Fig. 9.3) or less commonly on the forehead, upper eyelids, cheeks and nose. The mucosa is not involved [5]. ABNOM typically affects middle-aged Asians, particularly Chinese and Japanese, with age range of 20–70 years [1, 5]. They are thought to increase in thickness with advancing age [6].

Fig. 9.3
Speckled brown-gray macules on the malar regions in an Asian patient (Courtesy of the National Skin Centre, Singapore)
9.4 Solar Lentigines
Solar lentigines are characterized by well-circumscribed 1–3 cm pigmented macules on sun-exposed areas [7, 8]. They can occur in children and adults, especially those with skin types I to III.
Children who have xeroderma pigmentosum may develop solar lentigines in the first 6 months of life, after minimal sun exposure. Lesions may vary in color from light yellow to dark brown. The most common sites of predilection are the face (Fig. 9.4), hands, forearms, chest, back and shins.

Fig. 9.4
Dark brown patch on the cheekbone area of an Asian patient (Courtesy of the National Skin Centre, Singapore)
9.5 Drug-Induced Hyperpigmentation
Hyperpigmentation caused by toxic agents or medications (Fig. 9.5) accounts for 10–20 % of all cases of acquired hyperpigmentation. The most common causes are CNS drugs (e.g, chlorpromazine, amitriptyline), antineoplastic agents (e.g., carmustine, nitrogen mustard, bleomycin, anthracycline, 5-fluorouracil), anti-infectious drugs (e.g., chloroquine, quinacrine, hydroxychloroquine, minocycline, clofazimine, zidovudine), antihypertensive medications (e.g., amiodarone, diltiazem) and hormones (e.g., oral contraceptives) [1, 5].

Fig. 9.5
Bluish pigmentation on the face of a Filipino female, developed from intake of minocycline (Courtesy of the Research Institute for Tropical Medicine, Philippines)
9.6 Actinic Lichen Planus
It is a rare variant of cutaneous lichen planus, characterized by the development of lesions on the photodistributed areas (Fig. 9.6a). It is more common in dark-skinned populations, particularly in young adults [9]. Indurated plaques or papules appear on the face, neck and the dorsal surface of hands after exposure to ultraviolet (UV) light [10–12]. Covered areas and mucous membranes are usually spared. In few cases, discrete, confluent papules and hypermelanotic patches, sometimes assuming a melasma-like appearance (Fig. 9.6b), may also be seen. The etiology is unknown.
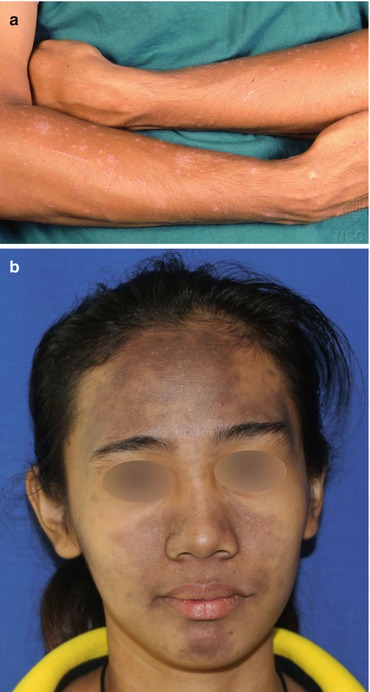
Fig. 9.6
(a) Scaly papules on the arms of an Asian male, histopathologically proven as actinic lichen planus (Courtesy of the National Skin Centre, Singapore). (b) Hypermelanotic patches on the midface of a young Filipino female, histopathologically proven as lichen planus (Courtesy of the Research Institute for Tropical Medicine, Philippines)
9.7 Erythema Dyschromicum Perstans (Ashy Dermatosis)
Erythema dyschromicum perstans (EDP) is a slowly progressive disease that is more common in children and young adults, particularly those from Latin America with skin phototypes III and IV [5]. It has equal prevalence in both sexes [1]. The common sites of predilection are the neck, proximal upper extremities and trunk [5]. Lesions can follow skin cleavage lines [3]. EDP is characterized by hyperpigmented macules and patches of variable shape and size with an ashen-gray to brown–blue color (Fig. 9.7) [13]. A polymorphic eruption may also be seen, presenting as simultaneous hypo- and hyperpigmented macules [14]. The lesions are usually asymptomatic; however, minimal pruritus can be present. There is a slow progression of the lesions over several years, usually without spontaneous regression.
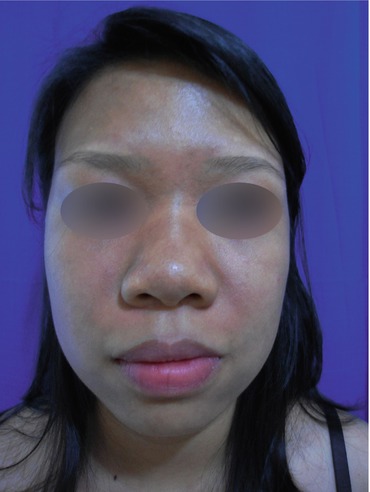
Fig. 9.7
Ashen-brown hyperpigmentation seen on the face of a young Filipino female (Courtesy of The Research Institute for Tropical Medicine, Philippines)
9.8 Riehl’s Melanosis
Also known as female facial melanosis, this condition is more common in middle-aged dark-skinned women, particularly Mexicans and Asians [1]. It is characterized by a rapid onset of a reticular gray-brown to almost black hyperpigmentation on the face (particularly on the forehead, zygomatic area and temples) and neck (Fig. 9.8a, b). There is no evidence of any inflammation on the skin [15]. It is induced by repetitive contact with a sensitizer such as fragrances, some pigments and bactericides (carbanilides, ricinoleic acids) used in cosmetics and optical whiteners [16].