Differential points
Infantile eczema
Childhood atopic dermatitis
Adult atopic dermatitis
Synonymous
Infantile seborrheic dermatitis
Prurigo Besnier
Infantile xerotic eczema
Atopic diathesis
Unknown
Yes
Unknown
Clinical manifestations
Localized to the scalp and face
Generalized distribution
Onset at puberty, seborrheic area
Flexor site of the extremities
Atopic red face, poikiloderma of the neck
Dry skin
Erythrodermic change
Laboratory data
NP
Elevated IgE-RAST to food allergens
Elevated serum IgE, TARC
Decreased IFN-γ production by umbilical blood
Elevated IgE-RAST to mite or pollen allergens
Increased IL4/IL5 production by umbilical blood
Positive patch test to metals, soaps, etc.
Elevated phosphodiesterase in monocytes
Differential diagnosis
Histiocytosis (Letterer-Siwe disease)
Hyper-IgE syndrome
Contact dermatitis
Psoriasis
Mastocytosis
Xerotic eczema
Contact dermatitis
Scabies
Seborrheic dermatitis
Infantile xerotic eczema
Miliaria
Pityriasis versicolor
Netherton syndrome
Ichthyosis
Hand eczema
Wiskott-Aldrich syndrome
Strophulus
Chronic actinic dermatitis
Juvenile dermatomyositis
Mycosis fungoides
19.2 Differential Diagnosis of Atopic Dermatitis
- 1.
Symptoms Associated with Sweat or Sebum
Infantile seborrheic eczema (Fig. 19.1, left top and bottom) is frequently observed on the head and face in infants. For diagnosis of AD, continuous observation of this eczema for longer than 2 months in infanthood or longer than 6 months in childhood is important [1, 2]. Observation of generalized eczema, fissured-ear base lichenification, randomly appearing dry skin, or association with atopic predisposition may be signs of transition to AD. In addition, in the summer season when sweating is promoted, serous papules or vesicles on the extremities or body trunk are occasionally observed (Fig. 19.1, center top and bottom) [3]. Hand eczema is observed in relation to irritation by sand or sweating (Fig. 19.1, right).
- 2.
Congenital Ichthyosis, Pediatric/Infantile Dry Eczema
Although Uehara et al. reported that 15% of observed AD patients were complicated with ichthyosis vulgaris [4], there are also some single cases. In the winter season, scalelike cornified lesions are clearly observed (Fig. 19.2, left). Expression of ceramide 10 and filaggrin 11 decreases in skin with atopic dermatitis, particularly in lesions, and is considered as a primary cause of barrier dysfunction [5, 6].
This is also considered as a secondary phenomenon associated with inflammation and as a cause of atopic dermatitis. Patients with the above symptoms should be carefully treated because steroids have no effects on dry skin and instead disrupt skin barrier function [7, 8]. In winter, as children’s skin is dry and pityroid dander is sometimes observed, these symptoms are referred to simply as dry skin (Fig. 19.2, center) or pediatric dry eczema. In some cases, the symptom of “pityriasis alba” may be observed. In psoriasis, circular keratotic erythema with white colored scales is observed. In infant patients, these lesions are frequently observed on the hip and sometimes such lesions are referred to as “diaper psoriasis” (Fig. 19.2, right).
- 3.
Scabies
Scabies is transmitted from the care stuff at elderly hospitals in many cases but also may be transmitted from pets such as dogs or cats (canine scabies). Symptoms are mainly pruritic lesions, in which exacerbation or delay of healing are observed in response to topical steroid application (Fig. 19.3). This disease causes family infection. It should be noted that in some dog, cat, or pediatric patient cases, no skin eruptions are observed on the predisposition site. Diagnosis is confirmed by microscopic tests to visually confirm the scabies worm white arrows or its eggs. Treatment should be guided by specialists.
- 4.
Mast Cell Disease
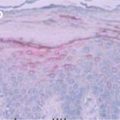
Mast cell disease is also called “urticaria pigmentosa,” in which sporadically occurring brownish pigment macules or papules are observed, mainly on the body trunk. Large numbers of mast cells are observed on the upper cutis, and urticarial lesions are shaped on pigment macules (Darier’s sign) by scrabbling. In some cases, histiocytosis X should be excluded because of positive CD1a staining [9].
- 5.
Pediatric Strophulus (Acute Prurigo)
In pediatric strophulus, large numbers of erythemas similar to urticaria occur after insect bite by mosquito, blackfly, etc., and sometimes shift to solid prurigo (known as strophulus) (Fig. 19.4). These symptoms frequently occur on all four limbs in the summer season. Eczema on intertriginous areas usually found in AD patients is not observed in this case. The symptoms are relieved by topical steroid application and oral administration of antihistamine drugs.
- 6.
Contact Dermatitis, Photocontact Dermatitis
Contact dermatitis or photocontact dermatitis is sometimes observed in response to moisturizing agents, topical drugs, soaps, shampoos, etc. These symptoms may appear similar to refractory lesions of AD but rapidly disappear by discontinuation of causative agents and topical steroid application (Fig. 19.5, left). In cases where the causative agents are unknown, the effects of topical steroids will gradually decrease and symptoms will become refractory. Diagnosis should be made by patch tests (contact dermatitis) or photopatch tests (photocontact dermatitis). An example of positive response in the patch test is shown in Fig. 19.5, center, with the suspected soap and shampoo in Fig. 19.5, right.
- 7.
Connective Tissue Disease
Childhood dermatomyositis is especially important in this disease. Erythemas on the face or body trunk or keratotic erythemas on the backside of joints are usually observed. In some cases, itching accompanies these erythemas with elevation of the serum IgE level [10, 11]. The patient shown in Fig. 19.6, left and right, was diagnosed with AD in childhood, and the picture in the center of Fig. 19.6 shows the clinical picture taken at the period of adolescence after growth. In this picture, calcareous depositions are observed.
- 8.
Histiocytic Disorders
Erythemas or papules associated with bleeding or other characteristic events are observed on the face, head, and body trunk (Fig. 19.7, upper, Langerhans cell histiocytosis). Pathological tests should be carried out to make a differential diagnosis. In this disease, CD1a is positive and Birbeck granules are observed by electronic microscopy (Fig. 19.7, lower pictures). In severe cases, chemotherapy should be conducted.
- 9.
Immune Deficiency Disease
In some cases of severe combined immune deficiency (SCID), erythemas or papules with dry pityroid dander are observed over the entire body. In Wiskott-Aldrich syndrome, eczema lesions similar to AD are observed. Netherton syndrome is characterized by ichthyosis, atopic diathesis, eczematous skin lesions with bamboo hairs, and SPINK5 gene mutation [12]. Hyper-IgE syndrome is a hereditary immune deficiency syndrome characterized by atopic dermatitis-like skin lesions, cold abscesses and pulmonary cysts with increased serum IgE and associated with STAT3, TYK2, or DOCK8 gene mutation [13].
- 10.
GVHD (Graft Versus Host Disease)
- 11.
Dermatitis Caused by Japanese Cedar Pollen
During the season when Japanese cedar pollen is released, typically from February to March in Japan, itchy urticaria and scaly dermatitis are observed on the face, especially around periorbital and nostril areas or the neck in some patients (Fig. 19.9, left). In AD patients, this is also important as one of the seasonally exacerbated factors [15, 16]. Patients with a history of aggravation of dermatitis exhibit positive delayed-onset scratch-patch tests to cry J1 (Fig. 19.9, right).
- 12.
Cutaneous T-Cell Lymphoma
It is important to differentiate mycosis fungoides from AD. In adult cases of AD, pruritic erythematous plaques or dirty poikilodermic lesions are occasionally observed with topical glucocorticoid resistance (Fig. 19.10, left and upper right). Histopathological evaluation (Fig. 19.10, lower left) using immunohistochemical analysis is recommended for differential diagnosis [17, 18].Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree