CHAPTER 9 DIEP Flap Breast Reconstruction
Summary
The lower abdominal region has evolved as the workhorse donor site for use in breast reconstruction. In particular, the deep inferior epigastric artery perforator (DIEP) flap has become popular in the hands of microsurgeons because of the balance between protection of the donor site and reliability for autologous breast reconstruction. The transverse rectus abdominis myocutaneous (TRAM) flap for breast reconstruction was first described by Holstrom1 and Robbins.2 It was Koshima and Soeda3 who brilliantly transformed this into a flap with complete muscle preservation, now known as the DIEP flap. When compared with the traditional pedicled TRAM flap, the DIEP flap has a lower incidence of fat necrosis or partial flap loss and has a lower incidence of hernia and abdominal bulge rates. When compared with the free TRAM flap, the DIEP flap, when properly raised, preserves all muscle function and abdominal fascia so that hernia and bulge rates are again lower4 and flap success rates are comparable. It should be noted that as the free TRAM flap has evolved to become more muscle-sparing, these structural abdominal donor site differences may be less.5 While the superficial inferior epigastric artery (SIEA) flap maintains the privilege of absolutely no violation of the abdominal wall, it cannot be carried out in all patients because of anatomical absence of the SIEA. Furthermore, the SIEA may not be able to reliably supply as much of the lower abdominal tissue for transfer as the DIEP flap, and failure rates in reported series are higher than for DIEP flap reconstruction. Although the DIEP flap appears to provide an ideal balance between reliability and low donor site morbidity, successful breast reconstruction using the DIEP is multifactorial, and proper patient selection and intraoperative decision making is essential.
Patient Selection
It has been shown repeatedly that obesity (body mass index, BMI > 30) and smoking result in increased rates of fat necrosis in the breast reconstruction and increased donor site complications.6–11 Patients should stop smoking a minimum of 3 weeks prior to elective flap surgery. There should be sufficient lower abdominal tissue to provide adequate volume for the breast reconstruction.
Scars in the lower abdomen require careful consideration. With appropriate perforator selection, there should be no increase in rate of total or partial flap loss or fat necrosis rate. However, the extent of intramuscular scarring that may interfere with perforator dissection may extend for a greater distance than can be appreciated by the external linear skin scar and it cannot be detected on preoperative imaging that may be used to map out dominant perforators. Furthermore, pre-existing abdominal scars may increase the incidence of donor site morbidity, with greater chance of wound breakdown, seroma, and abdominal bulge or laxity.12 Although abdominal liposuction is regarded by some as a contraindication to elevation of a DIEP flap,13 a series of DIEP flaps in abdominal liposuction patients has been successfully carried out after preoperative Duplex Doppler imaging.14 However, the newer modality of laser-assisted liposuction which is geared towards coagulating vessels and tightening the dermis has not been included in this study group and based on the mechanism of action, this form of liposuction would cause more damage to vessels than would traditional liposuction and should be considered a contraindication. Cosmetic abdominoplasty should also be considered a contraindication to elevation of a DIEP flap. A further discussion on avoiding complications when abdominal scars are present can be found in the Pitfalls section of this chapter.
Operative Technique
Surgical anatomy
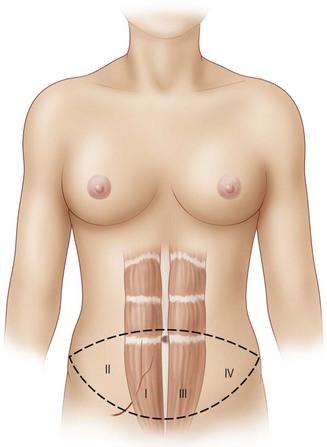
For free flaps, the best perfusion of the lower abdominal skin and fat is on the hemi-abdomen ipsilateral to the pedicle of the flap, as opposed to the central portion of the abdomen across the midline.15 This has been recognized to be the case both clinically and in anatomical dissections of DIEP flaps that have demonstrated variability in the presence of crossing branches of the venous plexus across the midline.16 It has also been supported by the work of Taylor investigating angiosomes.17,18 Therefore, Zone I constitutes the area directly over the ipsilateral rectus abdominis muscle from which the pedicle will arise, and Zone II lies lateral to the ipsilateral rectus abdominis muscle. Zones I and II constitute the ipsilateral hemiabdomen with the best zones of perfusion. Conversely, the contralateral hemiabdomen is composed of Zone III (the area adjacent to Zone I which lies across the midline, overlying the contralateral rectus abdominis muscle) and Zone IV is the remaining portion lateral to the contralateral rectus abdominis muscle which is furthest from the blood supply of the flap (see Fig. 9.1).
Elevation of a DIEP flap necessitates dissection through the rectus sheath as well as through a variable amount of rectus abdominis muscle because its source vessel, the deep inferior epigastric artery, arises from the external iliac artery deep to the inguinal ligament. The deep inferior epigastric artery is accompanied by paired venae comitantes. It pierces the deep surface of the rectus abdominis muscle as it ascends towards the umbilicus most commonly in the middle third (78%) and less commonly in its lower third (17%) or upper third (5%).19 It also has a variable branching pattern within the muscle. The deep inferior epigastric artery most commonly divides into a dominant lateral branch with an additional medial branch (54%). However, it may have a central course with multiple small branches (28%) or a dominant medial branch (18%).20 Both the level at which the deep inferior epigastric artery pierces the deep surface of the muscle and its branching pattern have implications for the difficulty of dissection of the DIEP pedicle, and this is where some of the variability and the learning curve in perforator selection arises. Although there are between two and eight perforators greater than 0.5 mm in diameter that pierce each side of the anterior rectus fascia in the paraumbilical region between 2 cm cranial and 6 cm caudal to the umbilicus and between 1 and 6 cm lateral to the umbilicus,21 perforators that are lateral tend to have a more direct perpendicular course through the muscle. Medial perforators, however, may have a long, complicated and oblique intramuscular course with numerous subsidiary muscular branches along the way. This is why preoperative imaging may be helpful in predetermining which perforator, if they appear to have comparable caliber where they are piercing the rectus abdominis fascia and entering the flap, would result in a technically easier pedicle dissection with potentially less disruption of the muscle during the dissection. However, it is also important to note that a more medial perforator may be more likely to supply a greater portion of the flap on the contralateral side of the abdomen.22
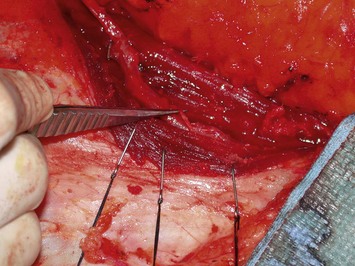
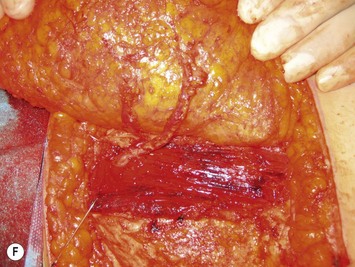
The relationship of nerves relative to the intramuscular course of the deep inferior epigastric artery is also an important consideration. Lateral perforators tend to be accompanied by larger sensory segmental nerves (see Fig. 9.2), which can potentially be used to neurotize the DIEP flap if an appropriate donor nerve in the mastectomy site can be located for neurorraphy. Motor nerves from intercostal contributions tend to cross superficial to the main branches of the deep inferior epigastric vessels (see Fig. 9.3) so that they can potentially be carefully dissected off of the main pedicle. However, because the motor nerves are segmental and travel in an oblique direction, they are often found traveling between sets of perforators arising from the same medial, lateral or central intramuscular row of the deep inferior epigastric. The implication here is that if two or more perforators in a row are used as the pedicle for the DIEP flap, then intervening segmental motor nerves need to be divided for removal of the flap.

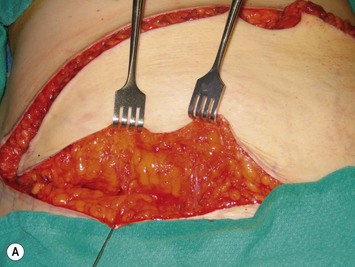
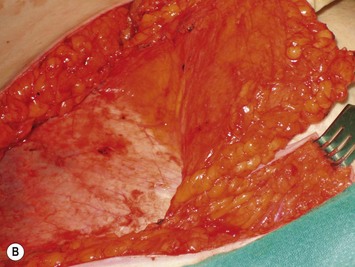
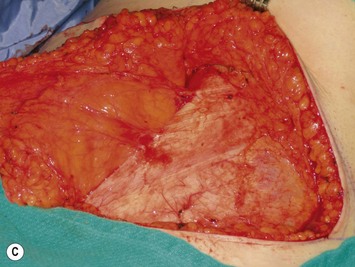
Finally, venous drainage may not be reliable. This is of particular concern for drainage across the midline. In some patients, the superficial venous drainage system may be dominant so that knowledge of the vascular anatomy of the superficial system is also important for DIEP flap elevation. Although a full description of the anatomy of the SIEA is found in Chapter 10, the essentials of the accompanying venous drainage system anatomy is highlighted as it relates to DIEP flaps. The landmark for the location of the SIEA – when it is present – at the level of the inguinal ligament is the midpoint between the anterior superior iliac spine and the pubic bone, or slightly lateral to this point,23 superficial to Scarpa’s fascia. It is accompanied by venae comitantes that travel inferiorly, piercing the cribiform fascia to descend to drain into the femoral vein. However, there is an additional superficial draining vein (medial epigastric vein) that is often present several centimeters medial to the artery which is often larger than the venae comitantes of the SIEA. Both the SIEA and accompanying venae comitantes and medial epigastric vein are shown in Figure 9.4A. This vein can be used as an alternate or adjunctive venous drainage for a DIEP making it essential that it be identified, dissected, and preserved if present. If a large vein from the superficial inferior epigastric system is encountered during flap elevation, this can be taken as a warning that drainage through the small perforating veins may be inadequate (see Fig. 9.4B and C).
Preoperative planning
Assessment of the perforator size and course can be carried out in advance with Duplex Doppler, computed tomography angiography (CTA), or even magnetic resonance angiography (MRA). If these modalities are not available, then surface handheld Doppler assessment can be used as a guide but it does not correlate as well to the exact location of where the perforator is piercing the fascia and it cannot delineate the vessel’s course. In contrast, Duplex Doppler scan of the lower abdominal wall can provide information on the position, flow, and diameter of the intramuscular perforators and can also be used to determine if the SIEA is present. A grid centered on the umbilicus and marked out in x– and y-axes at 1 cm intervals can be used to map the perforators and the grid can be laid out again on the day of surgery to localize the pertinent perforators. However, Duplex Doppler is operator-dependent and does not leave a permanent imaging record. In contrast, CTA can provide a permanent record of the preoperative roadmap for flap elevation.24,25 Dominant perforator locations can be measured on the images relative to the umbilicus, with these measurements then repeated on the patient and marked out on the skin surface. The intramuscular course can also be identified, so that the surgeon will know in advance which direction the perforator turns when it lies beneath the fascia, and whether it is lying just beneath the fascia or whether it plunges into the muscle. The length of the intramuscular course can be calculated and the branching pattern of the deep inferior epigastric vessels with which the perforator is associated can be determined. An example of CTA perforator mapping and clinical correlation is shown in Figure 9.5. Disadvantages of CTA include radiation dose and CT contrast that is administered during the study. To circumvent these disadvantages, MRA has been described to be used in a similar manner, but an MR image takes longer to perform than does a CT image. Preoperative imaging may also lead a surgeon to alter the limits of the markings of their donor site to a slightly higher location above the umbilicus in an attempt to have a greater amount of the flap centered on the selected dominant perforator. In addition, preoperative imaging may play a particular role in the case of extensive or unusual prior abdominal scarring where there is a question as to whether DIEA vessels are present or whether perforators exist to allow for DIEP flap elevation. Although each of the described imaging tools are adjuncts that have been shown in some hands to significantly decrease operative time and may be particularly useful for microsurgeons who are starting in practice, a DIEP flap can still successfully be elevated without their use based on intraoperative assessment, vascular anatomy knowledge, and meticulous technique. These fundamental principles apply even when the operating surgeon has preoperative imaging. There are very strong advocates of preoperative imaging, and similarly there are well-known experienced surgeons with equally successful outcomes who do not routinely obtain preoperative imaging. Thus, practice patterns vary and the surgeon should do what in his or her hands gives a successful outcome.

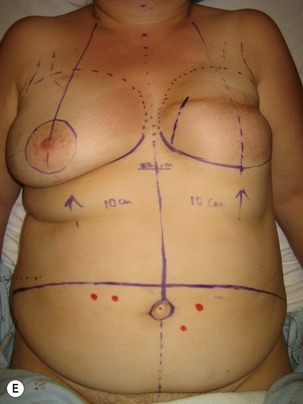

Preoperative markings are usually carried out in the standing position and confirmed once the patient is supine under anesthesia (see Fig. 9.5E). A fusiform ellipse is outlined on the lower abdomen that extends from the suprapubic crease inferiorly to just above the umbilicus superiorly and laterally to each anterior superior iliac spine (ASIS), although the territory may be extended to the midaxillary line.26,27 The amount of tissue that can be taken and still allow for closure of the donor site should be estimated by pinching the tissues. The amount that can be incorporated depends on the patient’s tissue laxity. It should also be noted that scars above the umbilical level (midline, paramedian, or subcostal Kocher scars) allow for less excursion of the remaining abdominal skin for closure. When one is attempting to maximize the amount of tissue that can be taken and it is suspected the closure may be unduly tight, the lowest portion of the marked ellipse can be adjusted in the operating room after elevation of the upper abdominal skin from above the umbilicus to the xiphisternum, followed by flexing the OR table at the patient’s waist, testing the excursion of the upper abdominal flap, and then remarking the inferior portion of the ellipse. The thickest fat of the flap is in the superior portion of the flap where the perforators are also the largest, so that the overall volume of the flap that is lost by having to superiorly adjust the inferior flap cut is usually not substantial and this maneuver can prevent abdominal wound problems even though it may add to the operative time.
Procedure
Mastectomy site and vessel preparation
In the case of an immediate reconstruction, mastectomy flaps should be assessed for hemostasis, viability, and extent of dissection. Any clearly non-viable areas should be excised to avoid the complication of mastectomy flap necrosis. If there is uncertainty and large areas are in question, modalities such as fluorescein imaging can be used or alternatively a delayed definitive flap inset can be carried out with the patient being returned to the OR approximately 48 hours later for excision of demarcated necrotic mastectomy skin flaps and de-epithelialization of the parts of the flap to be buried and final inset.28 Any overdissection of the mastectomy site, which most commonly occurs inferiorly or laterally, should be addressed with internal tacking sutures to recreate the inframammary fold and the lateral breast contour. The latter is an often underemphasized and very important aesthetic line of the breast, and it avoids having a large volume of the flap fall out laterally while helping to achieve medial fullness for cleavage and for masking of an internal mammary vessel recipient site.
Recipient vessels are prepared. The author’s preference is to use the internal mammary system as opposed to the thoracodorsal vessels. Use of the thoracodorsal vessels often results in more difficulty in medialization of the breast reconstruction flap and often more lateral breast fullness results (see Fig. 9.6A), although this can be addressed by maintaining long length of the DIEP flap pedicle and placing internal tacking sutures to hold the flap in the appropriate position. Furthermore, in the case of a delayed reconstruction the axilla is often scarred and the thoracodorsal vessels are more prone to spasm as compared to the internal mammary vessels. Finally, if a sentinel node biopsy is carried out at the time of an immediate reconstruction, there is the possibility that a completion axillary dissection will need to be carried out in the postoperative time period if the sentinel node is positive for metastatic disease.29 The implications are that the oncologic breast surgeon would have to carry out the axillary node dissection with repositioned thoracodorsal vessels and the relatively fresh pedicle to the DIEP flap within the field. The internal mammary vessels offer the advantages of more medial positioning of the flap (see Fig. 9.6B), negative intrathoracic pressure which aids in venous drainage, more protection from scarring and radiotherapy in the case of a delayed reconstruction, and protection from manipulation should a completion axillary dissection be required at a later date in the case of an immediate reconstruction with sentinel node biopsy. Although the internal mammary perforators (shown in Fig. 9.7A) can be used if they are of adequate caliber, the main vessels are often a superior size match to the DIEA and their venae comitantes. There is evidence to suggest that the left sided internal mammary vessels are smaller and in particular the veins are more often smaller, paired vessels. Despite this, in most cases they are usually still usable as even a small vein has the added advantage of the negative intrathoracic pressure to aid in venous drainage. The thoracodorsal vessels or rarely even the cephalic vein or external jugular vein can be used as an alternate drainage system. The author’s preferred technique for exposure of the recipient vessels is to first select a rib cartilage that will be covered by the DIEP flap reconstruction when the patient would be in a standing position in order to avoid a visible chest contour abnormality as shown in Figure 9.8 and even visible indrawing of the site with respiration. This has lead to selecting a lower rib than originally described, usually the fourth costal cartilage. The other advantages of a lower position are that vessel dissection and microvascular anastomosis does not require as much retraction of the mastectomy skin flap resulting in fewer traction-related ischemic mastectomy flap issues and easier exposure; the internal mammary vessels at this rib are also on a level plane, whereas at the location of the second rib they start to dive deeper into the chest with the curvature of the chest as they head toward the mediastinum. Finally, if the recipient vessels are inadvertently injured in the course of their dissection or in the case of a takeback for revision of an anastomosis there is sufficient extra length available by dissecting out a higher rib interval. The removal of the fourth rib cartilage, with exposure in the third and fourth intercostal spaces can give more than 3 cm of vessel length. Exposure is further optimized once the internal mammary artery and vein are divided at the inferior portion of the fourth intercostal space and allowed to curve more laterally. Excising too inferior a rib cartilage can lead to more technical challenges. For instance, the ribs start to travel more obliquely with small intercostal space intervals so that less vessel exposure is obtained. Furthermore, the internal mammary vessels can become smaller, with a shorter distance before the intercostal branches are given off, requiring more hemoclips in the field of dissection close to the area of the vessels that will be transected for the site of the anastomoses.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


