Medical imaging has become critically important in the diagnosis and treatment planning of vascular anomalies. The classification of lesions into fast-flow and slow-flow categories, the identification of a soft tissue mass, and the determination of the extent of the lesions are all facilitated by the use of magnetic resonance imaging, ultrasonography, catheter angiography, and other imaging studies. The use of these imaging techniques in the diagnosis and assessment of vascular tumors, malformations, and combined malformation syndromes is discussed in this article.
Medical imaging has become critically important in the diagnosis and treatment planning of vascular anomalies. The classification of lesions into fast-flow and slow-flow categories, the identification of a soft tissue mass, and the determination of the extent of the lesions are all facilitated by the use of magnetic resonance imaging (MRI), ultrasonography, catheter angiography, and other imaging studies. Ultrasonography is typically the first-line imaging study for the evaluation of vascular anomalies in children because sedation is not required. MRI may be indicated for diagnostic confirmation or to better define the anatomy of the lesion. Computed tomography (CT) gives superior resolution for osseous lesions.
Vascular tumors
Infantile Hemangioma
Infantile hemangiomas are benign tumors composed of endothelial cells. These lesions follow a predictable clinical course of proliferation in infancy followed by involution, usually within the first 5 to 7 years of life. Most cases do not require imaging. If clinical features are atypical or the anatomic extent of the lesion must be determined, ultrasonography and MRI can be of use.
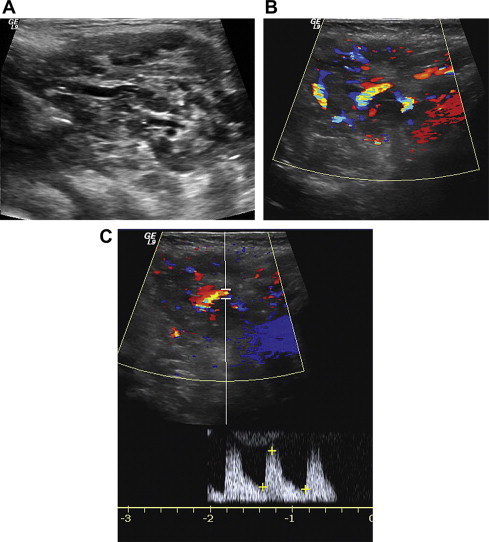
Typical ultrasonographic appearance of an infantile hemangioma, both in the proliferating stage as well as the involuting stage, is a well-circumscribed hypervascular mass showing low-resistance arterial waveforms ( Fig. 1 ). Most hemangiomas are hypoechoic, although up to 18% have been reported to be hyperechoic. Hemangioma can be differentiated from arteriovenous malformations (AVMs) by the presence of solid parenchymal tissue.
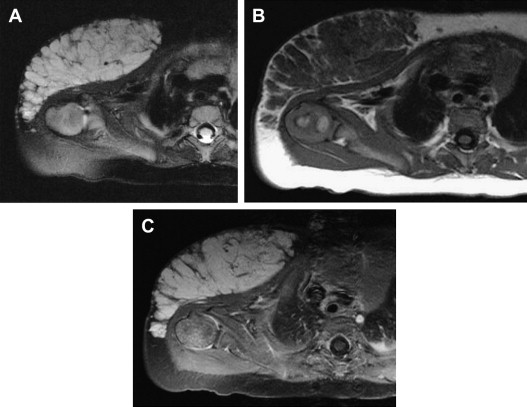
Proliferating infantile hemangiomas are lobulated hypervascular masses. On MRI studies, the lesions are isointense to muscle on T1-weighted sequences and hyperintense on T2-weighted sequences. High-flow central and peripheral vessels, seen as flow voids, are evident on T2-weighted sequences. After contrast administration, these masses enhance intensely and diffusely ( Fig. 2 ). In contrast to AVMs, arteriovenous shunting is not typically seen in infantile hemangioma.
During involution, infantile hemangiomas become more heterogeneous in appearance. MRI of involuting infantile hemangiomas demonstrates regions of fibrofatty deposition, manifested by areas of increased signal on T1-weighted sequences. Contrast enhancement diminishes and becomes inhomogeneous.
Rapidly Involuting Congenital Hemangioma and Noninvoluting Congenital Hemangioma
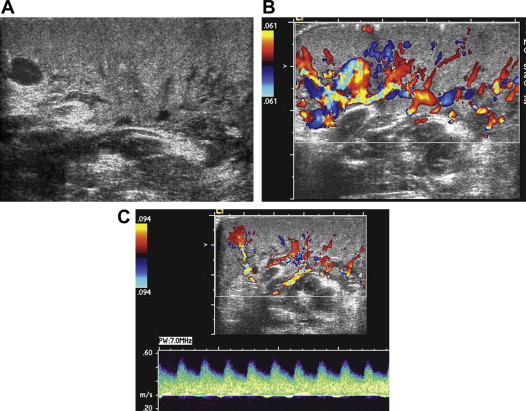
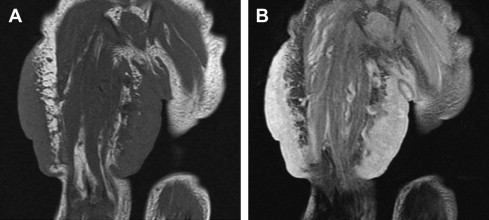
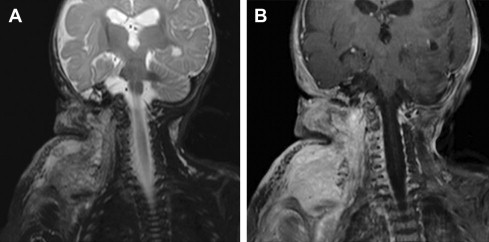
Congenital hemangiomas are tumors that have reached their maximal size at birth. Two variant forms of congenital hemangioma have been described: rapidly involuting congenital hemangioma (RICH) and noninvoluting congenital hemangioma (NICH). These lesions are distinguishable from infantile hemangioma by their clinical course, as described by their names. Unfortunately, these lesions cannot be reliably differentiated from common infantile hemangiomas based on imaging alone. However, some imaging features may be suggestive of a specific lesion. On ultrasonography, the useful differentiating factors are the presence of more visible vessels in congenital hemangiomas in comparison to infantile hemangioma, as well as the presence of intravascular thrombi, calcifications, vascular aneurysms, and arteriovenous shunting ( Fig. 3 ). RICH and NICH are less likely to be well defined than infantile hemangioma on MRI ( Fig. 4 ).
Kaposiform Hemangioendothelioma
Kaposiform hemangioendothelioma (KHE) is a rare vascular neoplasm with locally aggressive characteristics but without metastatic potential. MRI typically shows an ill-defined soft tissue mass that is hypo- or isointense on T1-weighted imaging and hyperintense on T2-weighted imaging. On administration of contrast, there is intense but heterogeneous enhancement ( Fig. 5 ). Subcutaneous fat stranding is an important feature that helps differentiate KHE from other benign fast-flow vascular masses. Prominent vascular channels, evidenced by flow voids, are usually present on MRI studies.
Vascular malformations
Lymphatic Malformation
Lymphatic malformations (LMs) are congenital malformations resulting from abnormal development of the lymphatic channels. The lesions may be classified as macrocystic, microcystic, or combined. On ultrasonography, macrocystic LM appears as a unilocular or mutilocular cystic lesion, usually with thin septations. Doppler imaging often demonstrates vascular channels within the septations. MRI of macrocystic LM shows clearly defined cysts that are hypointense on T1-weighted imaging and hyperintense on T2-weighted imaging. Fluid-fluid levels within the cysts may be present. The septa may enhance, creating a “rings and arcs” appearance ( Fig. 6 ). No flow voids or phleboliths are expected within the cysts.
Depending on the size of the cysts, microcystic lesions may appear as ill-defined hyperechoic masses on ultrasonography. Likewise, on MRI, microcystic LMs can appear as solid lesions that are generally hypointense on T1 sequences and hyperintense on T2 sequences. There is minimal enhancement on administration of contrast ( Fig. 7 ). Differentiation from soft tissue masses can be difficult. Categorization of LMs as slow-flow lesions and analysis of the extent of the lesions are two important tasks when imaging LMs.
Related posts:
 Vascular Anomalies: Current Overview of the Field
Vascular Anomalies: Current Overview of the Field
 Pathogenesis of Vascular Anomalies
Management of Venous Malformations
Pathogenesis of Vascular Anomalies
Management of Venous Malformations
 Management of Arteriovenous Malformations
Management of Arteriovenous Malformations
 Management of Combined Vascular Malformations
Management of Combined Vascular Malformations
 Special Considerations in Vascular Anomalies: Operative Management of Craniofacial Osseous Lesions
Special Considerations in Vascular Anomalies: Operative Management of Craniofacial Osseous Lesions
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


