CHAPTER 41 Dermal Suspension and Parenchymal Breast Reshaping after Massive Weight Loss

Summary/Key Points
Patient Selection
Breast deformities after massive weight loss vary significantly. Common findings include breast ptosis, medialization of the nipple–areola complex, and extension to a lateral chest roll. Many procedures exist to treat the deflated breast after massive weight loss, including short scar mastopexy techniques and combined augmentation/mastopexy.1–7 However, achieving long-lasting results with these techniques in the setting of severe skin laxity can be challenging. The goals for mastopexy after massive weight loss include obtaining a youthful, well-contoured breast with upper pole fullness, proper nipple positioning, and a long-lasting aesthetic result.
Patient goals and expectations must be properly assessed before proceeding with surgery. A full history and physical is always performed, with an emphasis on history of breast disease and analysis of the deformities. Optimal patient criteria for the dermal suspension, parenchymal reshaping mastopexy include profound parenchymal volume loss, skin envelope redundancy, Grade 3 nipple ptosis, medialization of the nipple–areola complex, and the presence of a lateral skin/fat roll or lateral chest wall laxity.8
Indications
As noted above, the indications for dermal suspension, parenchymal reshaping with selective auto-augmentation include patients with deflated, flattened breasts. Patients tend to have dramatic skin laxity and skin excess. Additionally, many patients present with lateral chest rolls of excess skin and/or fat,9 a nd this procedure is very effective in treating that deformity. The goals of this operation include using all available breast tissue and recruitment of surrounding chest wall tissue for selective auto-augmentation, proper placement of the nipple, restoring upper pole fullness, reshaping and reducing the skin envelope without relying on it for support, and eliminating the lateral chest roll and restoring the lateral sweep of the breast.
Relatively few contraindications exist for this procedure. Patients who are active smokers or users of tobacco products are asked to stop one month prior to and after surgery. In accordance with the American Cancer Society, all patients are screened for breast cancer with mammography as appropriate given their individual histories.10 Patients who have had prior breast surgery may not be candidates for this procedure if the scars interfere with the planned procedure. Similarly, patients with severe fibrocystic disease or active intertrigo may not be ideal for surgery. Patients desiring a marked increase in breast volume may be better served by an augmentation/mastopexy technique.
Operative Technique
Markings for the dermal suspension, parenchymal reshaping mastopexy are based on an extended Wise pattern with the nipple–areola complex based on a central and inferior pedicle. The sternal notch is identified and marked. A point on the clavicle 5 cm lateral to the sternal notch is identified and a line is drawn down the breast meridian. Often the nipple–areola complex in the massive weight loss patient will lie medial to this mark. The nipple position is then assessed by palpating the inframammary fold and projecting this point onto the surface of the breast. The top of the keyhole Wise pattern is planned from 2 cm above this point. Five centimeter vertical limbs are measured from the keyhole pattern. The Wise pattern is then completed with extension of the lateral portion to encompass the lateral skin roll. This will aid in removal of the skin roll and use of this de-epithelialized portion for selective auto-augmentation. The de-epithelialized portion is limited to the posterior axillary line and robust perforators from the lateral thoracic region allow the flap to be mobilized. The nipple–areola complex is measured at 42 mm with a cookie cutter or washer and de-epithelialization of the entire Wise pattern is begun (Fig. 41.1A).
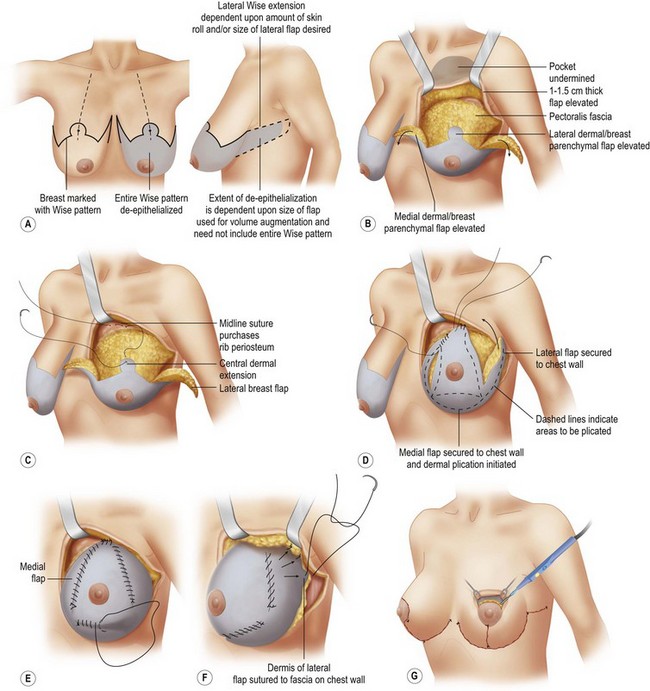
A pedicle base of 10 cm is measured approximately 6–7 cm from the medial aspect of the Wise pattern. All portions of the incision are then scored through dermis except at its base and the breast parenchyma is then raised as skin flaps with a thickness of 1 to 1.5 cm (Fig. 41.1B






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


