Microvascular free-flaps have changed reconstructive surgery. For patients undergoing maxillomandibular resections, free-flap surgery, especially use of the osseocutaneous fibula free-flap (FFF) has dramatically altered the ability to provide patients with good functional and aesthetic outcomes despite a large resection. The use of endosseous dental implants along with free-flaps has helped patients return to eating and speaking relatively quickly postoperatively. Implants can be placed primarily or secondarily depending on specific criteria. The Jaw in a Day concept has revolutionized providing patients with a rapid aesthetic and functional outcome for those undergoing maxillomandibular resections.
Key points
- •
Maxillomandibular reconstruction has been revolutionized by the Jaw in a Day concept.
- •
Jaw in a Day offers improved recovery, superior aesthetics and accelerated functional rehabillitation.
- •
Patient-specific implants and guides have allowed for faster and more patient specific rehabilitation.
Introduction
Free flap reconstruction and endosseous dental implants have significantly changed quality of life outcomes for patients undergoing maxillomandibular resections. Congenital defects, trauma, or pathologies involving the mandible or maxilla that require osseous resection can result in defects that are functionally and aesthetically challenging for patients. Fortunately, there have been significant advances in the reconstruction of these defects to rehabilitate patients. Reconstruction of postresective defects has been performed with a variety of techniques including autologous bone grafts, soft tissue and/or composite free flap reconstruction, and maxillofacial prostheses. Microvascular free flap reconstruction has become the standard for composite maxillofacial reconstruction because of improved outcomes.
There are many composite microvascular donor sites that have been described, with the most common sites being the fibula, ileum, and scapula. Reconstruction of the bony defect and soft tissues to provide adequate aesthetics and functional outcomes, particularly for mastication and speech, remains the primary means of maxillofacial reconstruction. The integration of virtual surgical planning and 3-dimensional prosthetic design led to the development of the Jaw-in-a-Day concept. This concept revolutionized the management for patients undergoing resection and reconstructive surgery. This approach allows for a predictable single-stage resection, reconstruction, and immediate dental rehabilitation with implant-supported prosthesis. For the patient, this offers an enhanced recovery, superior aesthetics, and accelerated functional rehabilitation.
Discussion
Choice of Free Flap
There are several bony free flaps that have been described in the literature including the most commonly used fibula (FFF), scapula (SFF) or iliac crest (ICFF), as well as radius, rib, femur, or metatarsal. Vascularized bone flaps have been shown to have better outcomes compared with reconstruction using soft tissue flap and plating. The choice of donor site depends on the amount of soft tissue, length of bone, and volume of bone required. Each donor site has its advantages and disadvantages. , , The most commonly used osseous free flap is the FFF, which was first described in 1989. There are many advantages of the FFF. It has been shown to be the most stable free flap over time with the least resorption compared with SFF or ICFF. Additionally, the FFF is much easier to harvest, allows for a 2-team approach, has a long pedicle, good length of bone, a skin paddle, and a consistent vascular anatomy. Furthermore, FFF has adequate cortical thickness, which is correlated with higher survival rates of the implants.
The biggest disadvantages of the FFF are the lack of vertical height and potential complications at the donor site including immobilization of the leg, the potential for vascular compromise of the foot, and the difficult closure, often requiring a split-thickness skin graft. ,
FFF and ICFF have appropriate bone volumes and stability over time (low resorption rates), making them ideal candidates for dental implantation. The ICFF provides a bulkier flap that can make swallowing more difficult; however, it is an appropriate option for mandibular and maxillary defects. Although all vascularized flaps have some level of donor site morbidity, the ICFF has been noted in the past for this disadvantage. The FFF is the preferred flap for patients requiring longer spans of bony reconstruction. The literature has shown there is an average survival rate of 93.5% of dental implants in FFF at the 1- to 5-year mark after implantation, with a survival rate of 80% after 10 years and 69% after 20 years postimplantation. , ,
Primary Versus Secondary Implants
Primary dental implantation involves placement of endosseous implants at the time of harvest of the free flap, whereas secondary implantation is usually performed around 4 to 6 months after free flap transfer. Primary dental implantation has several advantages through a single surgical procedure with the option for simultaneous insertion of dental prosthesis, offering an expediated form and functional recovery. , Some risks of implant placement at an osseocutaneous free flap include bone segment fracture, nonideal positioning and angulation of implants, inadequate insertional torque, and the undesirable possibility for tumor recurrence.
Secondary dental implantation requires a 2-staged surgical approach. The first surgery involves harvest and transfer of the free flap and placement within the defect with a reconstruction plate. After 4 to 6 months, the patient is brought back for implant placement. Secondary placement allows the surgeon to verify the integrity of the FFF and verify no evidence of disease or tumor recurrence. The 2-stage approach allows for the surgeon to orient dental implants to the neomandible anatomy and utilize patient-specific surgical guides for placement. If a skin paddle is present, flap debulking is often required to reduce the excessive thickness of tissue, and simultaneous vestibuloplasty may be required to optimize the soft tissue environment for dental rehabilitation. During the second stage, if a patient is radiated, care must be taken when incising the soft tissue surrounding the fibula so as not to damage any perforators. Drawbacks of the secondary implantation approach include inducing the patient to multiple surgeries, repeat exposure to general anesthetics, and the increased cost and delay in time to oral rehabilitation. In addition, patients will often suffer from diminished quality of life while waiting for prosthetic rehabilitation with a staged strategy.
Radiation Treatment
Patients with oral cancer who undergo mandibular or maxillary reconstruction may require radiation, which has been associated with higher rates of implant failure. This effect is dose dependent, and doses greater than 66 Gy have higher rates of implant failure compared with lower doses of radiation. For patients who undergo primary implantation, there is a risk in radiated patients of osteoradionecrosis of the fibula segment after re-entry to uncover implants. To prevent this, implants can be uncovered and vestibuloplasty performed 6 to 12 weeks after radiation is completed and before fibrosis occurs. For patients undergoing secondary implantation, the consensus is to wait around 6 to 12 months after completing radiation for implantation. ,
Methods for Implantation: Jaw-in-a-Day
Timely dental rehabilitation is critical to the functional, psychological, and social well-being of patients undergoing maxillomandibular free flap reconstructive surgery. The idea of Jaw-in-a-Day (JIAD) was first described in 2013 as a highly coordinated technique involving same-day resection, reconstruction, and dental rehabiltation. The ability to make this a 1-stage operation was revolutionized by the improved accuracy of virtual surgical planning and computer-aided design and computer-aided manufacturing technology. , The marrying of these technologies has allowed surgeons to virtually define resection margins, strategically plan osteotomy locations, and manipulate implant positioning to the patient’s anatomy. This approach allows for efficient, accurate, and predictable reconstruction with maximum patient aesthetic and functional outcomes.
The shape of the fibula varies along its length, with it taking on a more triangular shape at the head, quadrilateral in the middle, and more irregular near the malleolus. , In order to preserve as much length of the pedicle as possible, the middle to distal half of the fibula is often used. Virtual surgical planning and fabrication of titanium osteotomy and implant guides allow for precise placement within the bone stock, defined distances between implants, and orientation of implants. Although the FFF has good length, the lack of vertical height can be challenging to overcome depending on the necessary orientation of the FFF within the defect and the patient’s native anatomy. Double-barrel reconstruction or adjusting the placement of the fibula to 5 to 10 mm above the inferior border of the mandible can help in correcting the vertical height discrepancy. , The fibula bone must have at least 10 mm of height and 5 mm of width in order to support endosseous implants. , Similarly, appropriate vertical distance (15 mm) between the incisors is necessary to allow for dental implants. Appropriate placement of the reconstruction plate is important in order to prevent interferences between the implants and the fixation screws of the reconstruction plate. Using as few monocortical screws as possible for adequate fixation and stabilization of the plate is recommended. Implant placement in FFF is theoretically similar to placement in native bone. It is the experience of the authors that would advocate for bone tapping and overpreparation of osteotomies for dental implants. This accounts for the dense and cortical nature of the fibula compared with native mandibular bone, which can result in fracture of dental implants and/or the fibula bone. Care should be made to allow for attached soft tissue to remain around the implants so as to prevent peri-implantitis.
There are various implant-supported dental prosthetic configurations that can be used including conventional implant-supported bridge, resin-bonded bridge, implant-borne denture, and implant-stabilized denture. The type of prosthetic design is dictated by the patient’s occlusion and ability to maintain the prosthesis. This process is guided by the diligent involvement of a maxillofacial prosthodontist, who serves as the architect for the final prosthesis to ensure precise fit, optimal function, and biologic compatibility.
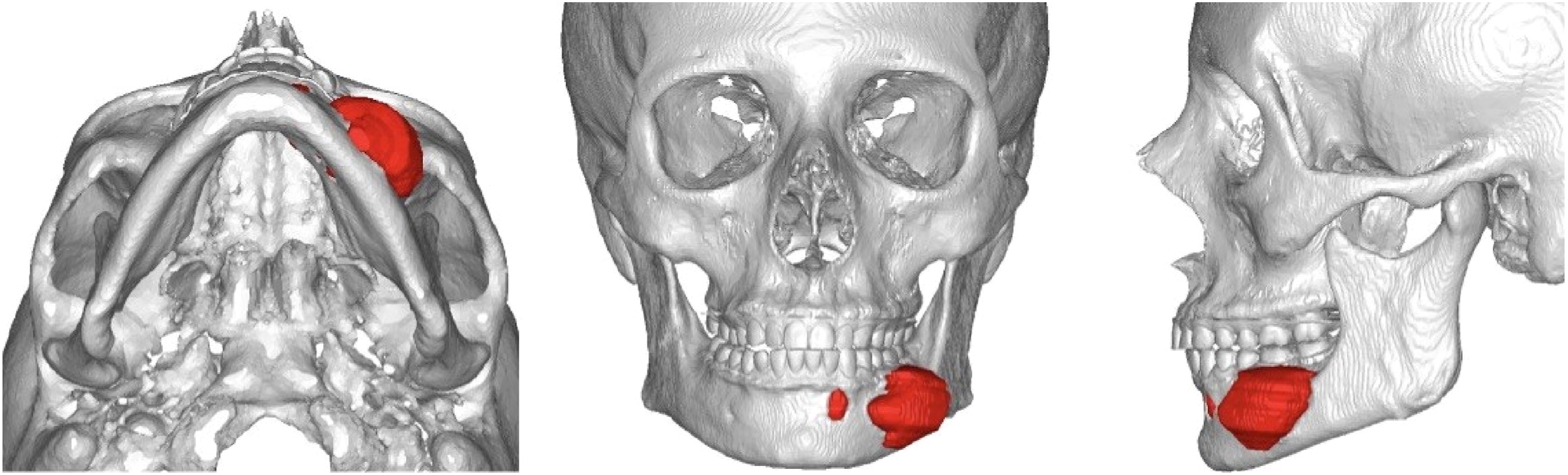
Benign pathology case
Figs. 1–9 explore the reconstructive process of a 36-year-old woman with biopsy-proven ameloblastoma of left mandible. Lesion shown in red.