15
Dental and Bony Architecture in Perioral Rejuvenation
Facial beauty is achieved when there is harmony between the size, shape, and position of all the elements in the face. Orthodontists and oral and maxillofacial surgeons use orthognathic principles based on lateral cephalometric radiographic evaluation to determine ideal facial proportions and bony positions. Orthognathic norms have been developed based on clinical and radiographic interpretation of the most aesthetically pleasing facial features of North Americans. Data obtained from patients with disproportionate facial components are compared with accepted orthognathic norms. Based on the deviation of the patient’s values from accepted norms, diagnoses of aesthetic deficiencies may be determined. Detailed evaluation from both profile and frontal views is always necessary for accurate assessment. All profile photographs and radiographs are taken with the patient in “natural head position.” A patient is considered to be in natural head position when the patient’s visual axis is parallel to a true horizontal plane (HP). This may be achieved by having patients look at the reflection of their eyes in a mirror. Alternatively, a line on the lateral cephalometric radiograph connecting porion (the external auditory canal) to orbitale (the infraorbital rim), commonly referred to as the Frankfurt horizontal (FH), may be used as true horizontal (Fig. 15-1 ).1 After the soft tissue and skeletal problems are identified, either orthodontic treatment, surgery, or a combination of both may be necessary to address the aesthetic needs of the patient.
The most beautiful face exhibits approximately equal vertical proportions of the upper, middle, and lower thirds of the face. The superior third is defined as the vertical distance from the trichal line (hair line) to nasion, which is the bony point separating the nose from the forehead. The middle third lies between the nasion and subnasale, the point where the nasal columella meets the upper lip. The inferior third lies between subnasale and the most inferior point on the chin.2
The lower third of the face, which is of most concern in the evaluation of oral and maxillofacial cosmetics, is further subdivided into the lower two thirds and the upper one third. The lower two thirds is composed of the lower lip and chin, and the upper one third consists of the upper lip.
The straight profile is considered most aesthetically pleasing according to arthropometric data obtained by Farkas and his colleagues from a population of young, North American adults.3 The profile is determined by the anterior-posterior positions of the maxilla, mandible, chin, and nose. If these bones are either too far behind or in front of a vertical line drawn through the nasion, the soft tissue profile appears either concave or convex, respectively, due to skeletal disproportions. In addition to being unaesthetic, a skeletal discrepancy may cause functional problems as a result of the teeth not fitting together properly. This discrepancy may cause difficulty with articulating speech, masticating food, or airway patency. Although some patients seek surgical correction of discrepancies of the facial bones for cosmetic reasons, others seek correction because of the resulting functional problems.
Harmony between the lower facial third and the rest of the face is achieved when the size, shape, and position of the teeth and bones underlying the facial soft tissues is balanced. Recognition of aesthetic abnormalities in the lower face will be discussed, and the link will be made to the etiology of the underlying dental and skeletal anomaly. Either or both surgical and orthodontic correction of these deficiencies based on accurate diagnoses will also be presented.
 Profile
Profile
Lip Projection
Determinants of the facial profile in the perioral region include the anterior-posterior position of the lips, mandible, and chin. Many methods have been described in the literature to illustrate the ideal lip position. One method is by using Rickett’s E-line. The E-line is a line drawn from the nasal tip to the anterior chin on soft tissue profile. Ideally, the lower lip should be 2 mm behind this line, and the upper lip should be 2 to 4 mm behind it.4 This method of evaluating lip position is limited because an excessively small chin or large nose can falsely predict abnormal lip position. Alternatively, we can use a vertical line perpendicular to FH through subnasale. Ideally, the upper lip should lie 1 mm anterior to, and the lower lip on the vertical line through subnasale (Fig. 15-1).1
Many factors influence lip projection. Lip thickness varies with age, gender, and ethnicity. Thick lips will be more prominent whereas thin lips will be less prominent. Protrusion of the teeth and jaws may cause the lips to be more projected whereas retrusion of the teeth, maxilla, or mandible may give the appearance of very thin lips. Size of the nose and chin on profile influences the perception of lip projection. Deficient chin projection may falsely give the perception of excessive lip protrusion. In addition, a large nose may falsely give the impression of deficient lip projection.
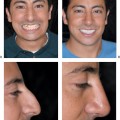
Clinical evaluation of the face, cephalometric analysis, and dental models are all helpful in determining the etiology of the lip projection problem and to distinguish true from perceived lip projection anomalies. Abnormal flaring of either or both the upper and lower teeth may cause excess lip protrusion. Teeth are considered flared when their inclination exceeds ideal. The ideal angulation of the upper incisors on profile is determined cephalo-metrically to be ∼110 degrees from the palatal plane. The ideal angulation of the lower incisors is ∼90 degrees to a line parallel to the inferior border of the mandible, or mandibular plane, on profile (Fig. 15-2).1 Excessive lip protrusion due to dental flaring with normal skeletal relationships may be reduced with orthodontic retraction of the anterior teeth combined with dental extractions of upper and lower premolars. Severe cases of bimaxillary (upper and lower jaw) protrusion that cannot be corrected with dental extractions and orthodontics alone may require maxillary and mandibular osteotomies to set back the jaws, in conjunction with orthodontic treatment (Figs. 15-3; 15-4). The surgically assisted movement of the jaws to achieve a straighter profile, in conjunction with orthodontics, is referred to in the oral and maxillofacial literature as orthognathic surgery.
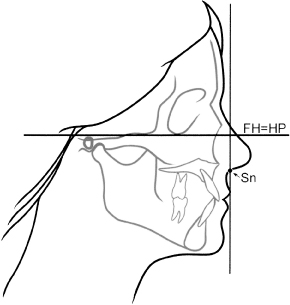
Figure 15-1 Lateral cephalometric tracing of facial bones and soft tissue profile. Frankfurt horizontal (FH), a line through the porion and orbitale is parallel to the true horizontal plane (HP). A vertical line perpendicular to the FH through the subnasale (Sn) demonstrates the soft tissue relationship of the lips and chin.
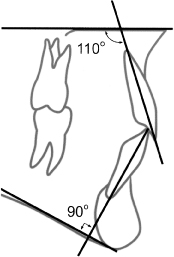
Figure 15-2 Ideal angulation of the upper and lower incisors. The angle between the palatal plane and upper incisor is 110 degrees. The angle between the mandibular plane and lower incisor is 90 degrees.
Patients with inadequate lip projection due to retrusion or severe crowding of the teeth may undergo orthodontics to flare, level, and align the teeth, which will improve lip projection. When lip projection is severely inadequate due to maxillary or mandibular skeletal hypoplasia, maxillary and/or mandibular osteotomies with advancement will improve lip projection and create a more harmonious profile. Patients who perceive subtle deficiencies in lip projection and whose teeth and jaws are in the appropriate positions may be candidates for lip augmentation procedures using fillers. These techniques are beyond the scope of this chapter, and are discussed elsewhere in Chapter 6.
Labiomental Sulcus
The labiomental sulcus is defined as the fold of soft tissue between the lower lip and chin. Form and depth of the labiomental sulcus may vary depending on the inclination of the lower and upper incisors, as well as chin projection. Cephalometric principles dictate that the ideal position of the most anterior point on the bony chin, the pogonion, should be about 2 mm behind a vertical line perpendicular to the FH through nasion.1 Position of pogonion and inclination of the incisors should both be measured when determining the etiology of labiomental sulcus anomalies.
For example, a prominent chin with severely proclined upper and lower incisors can create an unaesthetically deep mentolabial sulcus. Conversely, a prominent chin due to mandibular hyperplasia, or excess growth of the lower jaw, with retroclined incisors may give the appearance of a shallow labiomental sulcus.

Figure 15-3 Patient with excess lip protuberance from bimaxillary protrusion. (Courtesy of Dr. S. Roser, Emory, Atlanta, Georgia.)

Figure 15-4 Patient in Fig. 15-3 after maxillary and mandibular osteotomies with repositioning. Profile in the perioral region is straighter and more aesthetic. (Courtesy of Dr. S. Roser, Emory, Atlanta, Georgia.)
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


