Deltopectoral Skin Flap
V. Y. BAKAMJIAN
EDITORIAL COMMENT
This landmark chapter should be studied with considerable care and detail. The deltopectoral flap preceded the pectoralis major flap in head and neck reconstruction, and although it is not as reliable as the latter for intraoral resurfacing or in postradiation patients, the versatility and reach of the deltopectoral flap are admirable. Safety is ensured by preservation of the second perforating branch of the internal mammary artery and by flap design and subfascial elevation, as emphasized by the author.
INDICATIONS
With optimal flap reach occurring in stockier patients with broad shoulders and short necks, the flap may serve at almost any head and neck level below the ipsilateral eyebrow (Fig. 127.1) or below midlevel of the contralateral face, if necessary (Fig. 127.2).
ANATOMY
Two contiguous but separate axially vascularized zones are distinguishable in the area of the flap (Fig. 127.3), with or without a random narrow zone at the far end (16). Intercostal perforating branches from the internal mammary artery arborize outward in the pectoral zone; a cutaneous vessel from the thoracoacromial artery does the same in the deltoid zone; and a few musculocutaneous short twigs from the subscapular and circumflex humeral vessels pierce into the random distal zone. When the flap is elevated, however, its survival will depend entirely on the flow of blood in the branches from the internal mammary to the pectoral zone passing by means of rich dermal and subdermal plexus connections into the axially oriented vasculature of the deltoid zone and beyond. Clinical experience has amply demonstrated that the blood supply of internal mammary origin suffices for full survival of the flap, without delay, in 85% to 90% of patients.
FLAP DESIGN AND DIMENSIONS
Based parasternally over the three or four upper intercostal spaces, the flap extends horizontally to the anterior aspect of the shoulder, where its curvilinear distal margin may reach to the anterolateral, midlateral, or even posterolateral contour
line of the deltoid region, depending on specific case requirements (Fig. 127.4). It then can carry a generous portion of deltoid skin, not damaged by prior radiotherapy or compromised by incisions used in resecting head and neck cancer, on the end of a pedicle of pectoral skin.
line of the deltoid region, depending on specific case requirements (Fig. 127.4). It then can carry a generous portion of deltoid skin, not damaged by prior radiotherapy or compromised by incisions used in resecting head and neck cancer, on the end of a pedicle of pectoral skin.
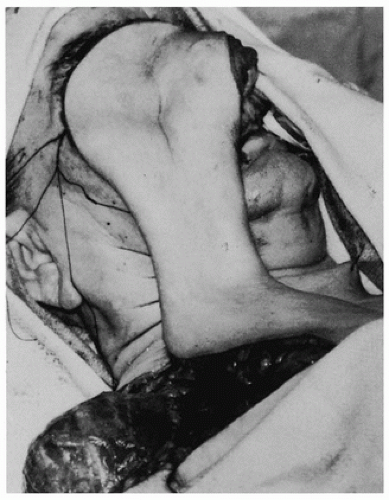 FIGURE 127.1 Ipsilateral high reach of the flap. |
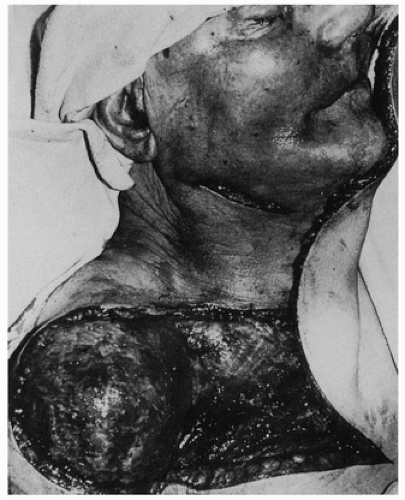 FIGURE 127.2 Contralateral reach of the flap. |
The actual reach of the raised flap is longer than would be surmised from its outlined dimensions when the patient’s arm lies by his or her side. This can be explained by the considerable elongation that characteristically occurs along the lower border of the flap as it is raised in cephalad rotation. The phenomenon is due to the better than average stretching ability of skin in the vicinity of the axillary fold—essential for the full range of abduction and elevation of the arm (Fig. 127.5). Consequently, the pivot point for rotation of the flap shifts from the lower to the upper medial corner of its base. Tilting the patient’s head toward the base of the flap also helps determine proper flap dimensions.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


