This article summarizes current information on the risk and the assessment of risks for deep venous thrombosis (DVT) resulting from plastic surgery procedures. Risk assessment is the foundation for recommended methods of prevention of DVT and, in turn, possible pulmonary emboli. If prevention fails, treatment of DVT is required to avoid the major complication of pulmonary emboli. The significant risk of DVT and pulmonary emboli after an abdominoplasty is confirmed in this article.
Key points
- •
Deep vein thrombosis and its possible sequela of pulmonary embolism are a major risk for plastic surgery patients.
- •
Patients undergoing an abdominoplasty are at a significant risk of death due to pulmonary emboli.
- •
Risk assessment is the basis for prevention of thromboembolic phenomena.
- •
Measures to prevent deep venous thrombosis must be taken based on risk stratification.
- •
Early diagnosis and treatment of deep venous thrombosis or pulmonary emboli are essential to decrease the risks of these serious sequelae.
The incidence of thromboembolic phenomena, including deep venous thrombosis (DVT) and its feared sequela of pulmonary embolism (PE), are major health care issues and known postoperative risks of lengthy surgical procedures. The Surgeon General’s Call to Action to Prevent Deep Vein Thrombosis and Pulmonary Embolism , 2008 estimated that 350,000 to 600,000 Americans suffer annually from DVT and PE and that at least 100,000 deaths per year may be related to these diseases. In 2009, the National Quality Forum had even more impressive statistics : each year more than 900,000 Americans form DVTs, of which 500,000 experience a PE, resulting in roughly 300,000 deaths. Surgeons who operate in ambulatory facilities must become aware of these health risks for their patients.
Overview
An historical review of the plastic surgery literature reveals studies that offer recommendations for both DVT prophylaxis and risk management, starting with a 1999 article by Noel McDevitt. The executive committee of the American Society of Plastic Surgeons (ASPS)–approved Venous Thromboembolism Task Force Report identified the best practices for DVT/PE prevention and treatment. The ASPS Task Force on Patient Safety has also published articles offering recommendations for DVT prophylaxis based on levels of risk in ambulatory surgery settings. The need for awareness of DVT/PE prophylaxis in plastic surgery, and specifically in liposuction and abdominoplasty procedures, has been the basis for numerous articles. The correlation of DVT/PE and body-contouring surgery after massive weight loss was addressed by Kenkel, for abdominal contouring by Hatef and colleagues, and is still receiving attention as documented by Egrari in 2012. The risk of DVT is even greater in patients receiving orthopedic care and in certain categories of trauma and general surgery than in plastic surgery. There is extensive published literature to support this conclusion.
Facelifts and their association with DVT/PE were documented by Rigg and by Reinisch and colleagues in 1998, and still remain an important topic, as pointed out in the article by Abboushi and colleagues in 2012. The facelift procedures that were complicated by postoperative DVT were performed under both local anesthesia with sedation and general anesthesia, continuing a long discussion as to whether avoidance of general anesthesia can decrease or eliminate DVT/PE. Hoefflin countered by reporting no major complications in 23,000 cases under general anesthesia.
American Association for the Accreditation of Surgical Facilities
Peer Review Data: September 2012
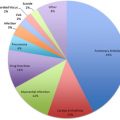
The American Association for the Accreditation of Surgical Facilities (AAAASF), through its quality assurance and peer review process, has previously reported on significant issues in ambulatory surgery. The latest data are shown in Table 1 and confirm the many reports that DVT/PE is a major problem for patients having plastic surgery. Of the 3,922,202 plastic surgery cases, there were 215 DVTs and 264 PEs for a total of 479. This is an incidence by case of 0.01222% or 1 in every 8188 cases. The largest number of venous thromboembolism (VTE), 308, occurred with abdominoplasties. The abdominoplasty procedures performed alone were 98; abdominoplasties plus 1 additional procedure were 137; plus 2 additional procedures, 58; and plus 3 additional procedures, 15, which is an incidence of 0.0666% or 1 in every 1502 cases. Total abdominoplasties that were associated with a PE were 185, with an incidence of 0.04% or 1 in every 2500 cases. The distribution of PE cases associated with abdominoplasty alone or abdominoplasties with multiple procedures is similar to the data for patients having VTE/PE. There is no significant statistical difference for VTE or PE whether the abdominoplasty is performed alone or with multiple other procedures. It has been reported in the literature that performing multiple procedures at the same time increases the risk of complications, such as VTE. These peer-reviewed data do not support that conclusion.
| Total Cases all AAAASF Specialties | 5,416,071 | ||||
| Total Procedures all AAAASF Specialties | 7,629,686 | 1.41 | Procedures per Case | ||
| Plastic Surgery Cases | 3,922,202 | ||||
| Plastic Surgery Procedures | 5,525,255 | 1.41 | Procedures per Case | ||
| Incidence % by Case | 1 in # Case | Incidence % by Procedure | 1 in # Procedure | ||
| All Deaths all Specialties | 184 | 0.0034% | 29,435 | 0.0024% | 41,466 |
| Incidence % by Plastic Surgery Case | 1 in # Plastic Surgery Case | Incidence % by Plastic Surgery Procedure | 1 in # Plastic Surgery Procedure | ||
| All Plastic Surgery Deaths | 94 | 0.0024% | 41,726 | 0.0017% | 58,779 |
| Total Abdominoplasties Performed | 462,564 | ||||
| Abdominoplasty Alone | 176,092 | ||||
| Abdominoplasty + 1 other procedure | 187,847 | ||||
| Abdominoplasty + 2 other procedures | 73,869 | ||||
| Abdominoplasty + 3 other procedures | 24,756 | ||||
| Incidence % by Case | 1 in # Case | Incidence % by Procedure | 1 in # Procedure | ||
| Total Plastic Surgery VTE | 479 | 0.0122% | 8188 | 0.0087% | 11,535 |
| Plastic Surgery DVT | 215 | 0.0055% | 18,243 | 0.0039% | 25,699 |
| Plastic Surgery PE | 264 | 0.0048% | 20,929 | 0.0048% | 20,929 |
| Incidence % by Case | 1 in # Case | ||||
| Abdominoplasty + VTE | 308 | 0.0666% | 1502 | ||
| VTE Abdominoplasty Alone | 98 | 0.0557% | 1797 | ||
| VTE Abdominoplasty + 1 other procedure | 137 | 0.0729% | 1371 | ||
| VTE Abdominoplasty + 2 other procedures | 58 | 0.0785% | 1274 | ||
| VTE Abdominoplasty + 3 other procedures | 15 | 0.0606% | 1650 | ||
| Incidence % by Case | 1 in # Case | ||||
| Abdominoplasty + PE | 185 | 0.0400% | 2500 | ||
| PE Abdominoplasty Alone | 60 | 0.0341% | 2935 | ||
| PE Abdominoplasty + 1 other procedure | 81 | 0.0431% | 2319 | ||
| PE Abdominoplasty + 2 other procedures | 37 | 0.0501% | 1996 | ||
| PE Abdominoplasty + 3 other procedures | 7 | 0.0283% | 3537 | ||
| Incidence % by Case | 1 in # Case | Incidence % by Procedure | 1 in # Procedure | ||
| Deaths PE All Plastic Surgery Procedures | 40 | 0.0010% | 98,055 | 0.0007% | 138,131 |
| Deaths PE Abdominoplasty Alone | 6 | 0.0034% | 29,349 | ||
| Deaths PE Abdominoplasty + 1 other procedure | 10 | 0.0053% | 18,785 | ||
| Deaths PE Abdominoplasty + 2 other procedure | 9 | 0.0122% | 8208 | ||
| Deaths PE Abdominoplasty + 3 other procedure | 1 | 0.0040% | 24,756 | ||
| Total Deaths PE Abdominoplasty | 26 | 0.0056% | 17,791 | ||
| Deaths Facelift and Blepharoplasty | 5 | ||||
| Deaths PE Liposuction | 5 | ||||
| Death PE Buttocks Thigh Extremity Lift | 2 | ||||
| Deaths PE Breast Augmentation or Lift | 2 |
Related posts:
 Conscious Sedation/Local Anesthesia in the Office-Based Surgical and Procedural Facility
Conscious Sedation/Local Anesthesia in the Office-Based Surgical and Procedural Facility
 Deep Vein Thrombosis Chemoprophylaxis in Plastic Surgery
Deep Vein Thrombosis Chemoprophylaxis in Plastic Surgery
 Airway Management in the Outpatient Setting
Airway Management in the Outpatient Setting
 Outpatient Surgery and Sequelae
Outpatient Surgery and Sequelae
 Management of Postoperative Nausea and Vomiting in Ambulatory Surgery
Preventing Surgical Mishaps
Management of Postoperative Nausea and Vomiting in Ambulatory Surgery
Preventing Surgical Mishaps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


