65
Cutaneous Manifestations of HIV Infection
There are a number of cutaneous disorders that point to the diagnosis of HIV infection. For some, it is the mere presence of the skin disease, whereas for others, the disease is extensive or proves recalcitrant to therapy (Table 65.1; Figs. 65.1–65.12). As HIV infection is associated with immunosuppression, the clinical presentation of various infectious diseases is often reminiscent of that observed in individuals whose immunocompromised state is due to medications (e.g. CS plus chemotherapy) or underlying diseases (e.g. acute leukemia).
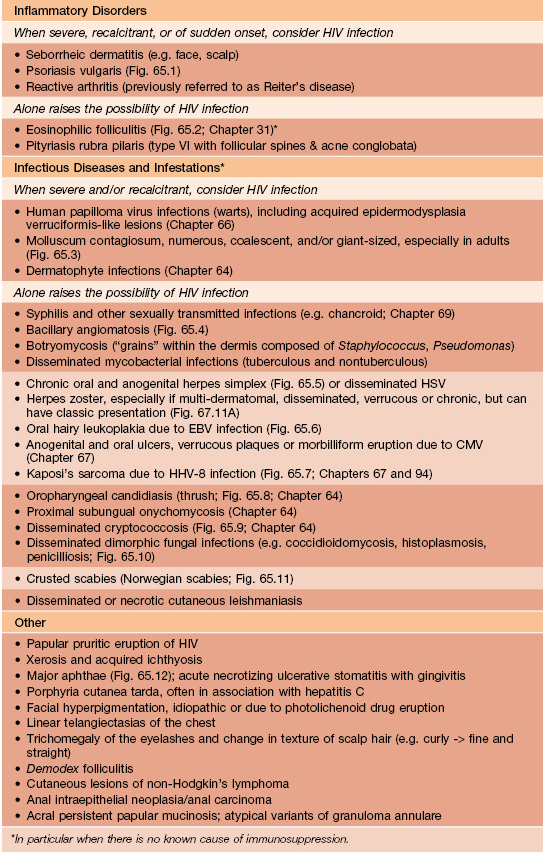

Fig. 65.1 Severe psoriasis in a patient with AIDS. Both sudden acute exacerbations and treatment resistance can be observed.

Fig. 65.2 Eosinophilic folliculitis. Due to associated pruritus, follicular papules are often excoriated; lesions favor the head and upper trunk. Courtesy, Clay J. Cockerell, MD.

Fig. 65.3 Molluscum contagiosum in the setting of HIV infection. Large lesions due to coalescence of individual papules. The face is a common location.

Fig. 65.4 Bacillary angiomatosis. Lesions can resemble vascular tumors or pyogenic granulomas and are a reflection of infection with Bartonella henselae or B. quintana.

Fig. 65.5 Chronic ulcerative herpes simplex viral infection in an HIV-infected patient. These slowly enlarging ulcers of the buttocks and perianal area have a characteristic scalloped border.

Fig. 65.6 Oral hairy leukoplakia. Shaggy white keratotic plaques along the lateral aspect of the tongue. A corrugated pattern is often seen. Courtesy, Charles Camisa, MD.



Fig. 65.7 Kaposi’s sarcoma in the setting of AIDS. Violaceous papules and plaques involving the face (A), palate (B), and an extremity (C). The patient also has oral candidiasis. C, Courtesy, Thomas Horn, MD.

Fig. 65.8
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


