Creating a refreshed, best version of an individual face requires knowledge of facial anatomy, understanding of the interactions of fillers and neurotoxins with tissue and muscle, and dedication to the primary principal of aesthetic responsibility. The forehead ages in a similar fashion to the rest of the face with loss of volume in both subcutaneous fat and bone. Different injection techniques are recommended for the forehead, midface, lip, and lower face. Although we understand the changes associated with aging from a global perspective, each individual ages at his or her own pace and in consideration to their specific anatomy.
Key points
- •
The forehead ages in a similar fashion to the rest of the face with loss of volume in both subcutaneous fat and bone.
- •
Different injection techniques are recommended for the forehead, midface, lip, and lower face.
- •
From an aesthetic standpoint the entire perioral area must be treated, meaning the cutaneous lip, as well as the commissures and the chin.
Introduction
In recent years, there have been significant advances in understanding the anatomy and physiology of the aging face. Although we understand the changes associated with aging from a global perspective, each individual ages at his or her own pace and in consideration to their specific anatomy.
For example, patients of Asian, Caucasian, Hispanic, and African descent demonstrate different changes in their anatomy as they age. When seen in the context of cumulative photodamage, some individuals see more descent and a thickening of their skin whereas others have more wrinkling and less descent. The overall shrinkage of the face that begins at the skeletal level extending to the superficial and deep fat pads and the skin envelope leads to unique alterations in the overall facial physiognomy. To provide optimal corrections to aging changes in the face, it behooves the treating physician to design an injection approach that addresses each individual based on their unique needs.
Evaluating the face in both a 2-dimensional and a 3-dimensional fashion is achieved using a combination of 3-dimensional imagery and calipers measuring the anatomic landmarks, such as the projection of the chin, the nose, the cheek, and the brow. The simplest clinical approach is to begin by dividing the face into thirds. The top third begins at the inferior aspect of the hairline, ending at the brow; the middle third begins at the brow and ends at the upper lip, and the lower third begins at the upper lip and ends at the chin and jaw line. This author likes to begin the process by first assessing the face as a single cosmetic unit and second, divide into thirds, and finally to use the phi principal of beauty to precisely determine how injections will ultimately deliver the optimal results in terms of reversal of aging and creating the most beautiful version of the person.
Assessment and treatment of the top third of the face
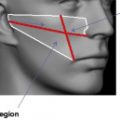
In a similar process to the entire face, the forehead flattens owing to loss of volume in both subcutaneous fat and bone. This leads to a skeletal appearance with flattening of the normal, pleasant youthful curve of the forehead, as well as prominence of veins that had not been visible in a younger face. The muscle responsible for lifting the brow and creating transverse wrinkles is the frontalis muscle, and in some individuals this motion creates deep horizontal lines in their forehead, Fig. 1 . Using newer techniques it is possible to safely revolumize the forehead in a judicial fashion. One technique is to use a hyaluronic acid product such as Juvéderm Ultra, Restylane, or Boletero blended with one-third volume of plain lidocaine. This mixture allows for easier spread when injected into the subgaleal/periosteal plane. This author prefers to use a BD needle with a 0.30 mL syringe allowing precision injecting of small, controlled boluses of material. One can inject 0.05 to 0.10 mL at different points in the central forehead, well above the glabellar region, and gently spread the material using massage. This maneuver reestablishes the youthful curvature and softness seen in a younger face. Another technique is to use a cannula to deposit the filler in the subgaleal plane along with massage. This author has found this procedure to be more difficult in this area. Revolumizing the medial brow is necessary to lift the brow and soften the horizontal lines of the forehead, and returns the forehead to a more youthful look.
Often, there is brow ptosis that occurs over time, owing to both bony loss, descent, and shrinkage of the underlying fat pad in the brow area. To reestablish the lift of the lateral brow, a combination approach using a neuromodulator such as, onabotulinumtoxinA, abobotulinumtoxinA or, incobotulinumtoxinA, along with a hyaluronic acid is used. To lift the lateral brow, first assess the glabellar muscular complex and the orbicularis oculi to determine how many units of toxin are required to relax this depressor complex and the type of frown that the patient makes. Then at the same time, or preferably at a second visit, the lateral brow can be injected, at the hairline just anterior or superior to the temporalis muscle, using anywhere from a 0.5 to 1 mL of either Restylane or Perlane because these agents are both slightly stiffer and provide more lift. In the temple, a blend of either 1.0 mL Juvéderm Ultra Plus or Perlane with 0.5 mL plain lidocaine is injected down to periosteum. For the lateral tail of the brow, injecting just underneath the dermis and into the subcutaneous fat pad using anywhere from 0.1 or 0.2 mL Juvéderm Ultra or Restylane, not blended so as to avoid diffusion of the product. Another nice technique is to use a cannula in the subcutaneous space beneath the tail of the brow.
The author recommends a judicial use of neurotoxin in the upper third of the face. The muscular complex that forms the glabellar region including the corrugators, procerus, and parts of the orbicularis oculi can be treated in a relatively low-dose fashion to avoid a frozen look. This author recommends evaluating the musculature to determine the number of units necessary to achieve a relaxed look.
For the brow area, once again the author recommends a more conservative approach to neurotoxin dosing to allow for more movement of the forehead. In the crow’s feet area, because the orbicularis oculi is very thin, this author treats where the patients muscle is contracting and use anywhere from 6 to 12 U.
Assessment and treatment of the midface
There has been an enormous step forward in the assessment and treatment of the midface. We now understand how the treatment of the midface impacts both the nasolabial fold and the commissures. Accurate treatment can deliver on the promise of beautifying the face by establishing a stronger projection of the malar eminence, maxilla, and curve of the cheek. With appropriate distribution of volume of product the skin envelope will redrape. In general, product placement is planned using Hinderer’s lines ( Fig. 2 ). The injection begins from the superior point of the malar eminence continuing onto the inferior maxillary zone. Injecting directly on top of the periosteum lifts up the superficial and deep fat pads. Injections are continued medially, as described by Montes and they define the midface and lower jawline.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


