This article presents the use of an intraoperative surgical guide created by 3D laser surface scanning and rapid prototyping. The authors present outcomes of 3 patients in whom the nasal surgical guide was used intraoperatively for reconstruction of full-thickness, complex nasal defects. This effort highlights the multidisciplinary approach involving a surgeon and anaplastologist integrated with the latest technology to provide patients with the best possible outcomes.
The reconstruction of total or subtotal nasal defects can be an extremely daunting task. It is essential to abide by the principles of nasal subunit anatomy and the 3 layers of reconstruction: vascularized inner lining flaps, rigid framework, and the external skin lining. The ideal is to reapproximate the original functional and aesthetic characteristics. The 3-dimensional (3D) nature of the nose requires careful attention to lifelike dimensions and surface contour while guarding against scar contracture and asymmetric healing. The accurate recreation of the 3D anatomy of the nose is fairly straightforward in most nasal defects created by skin cancer resections and trauma, because most defects spare the majority of the nose, such as the contralateral side. Thus there exists a visible 3D reference. The challenge is vastly greater in subtotal and particularly total nasal defects. When the entire nose (including the nasal septum) is removed, it is very difficult to envision accurately the 3D anatomy, including the accurate relationship of the nasal structures to the surrounding facial anatomy. Various strategies have been proposed to navigate the small margin of error for successful outcomes. The authors present their use of an intraoperative surgical guide for reconstruction of full-thickness, complex nasal defects, created by 3D laser surface scanning and rapid prototyping (RP). This guide increases the ease and accuracy of creating the subsurface framework and highlights the increasing role of technology in surgical advancement. The development of this sterile, translucent template requires the multidisciplinary team of a surgeon and anaplastologist in close cooperation with the patient.
Anaplastology
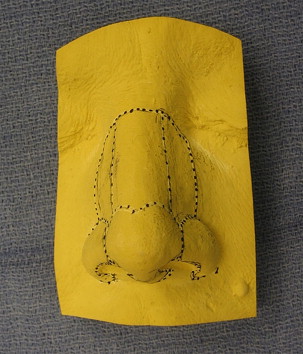
An anaplastologist specializes in the prosthetic rehabilitation of absent or disfigured aesthetically critical portions of the body such as the ear and nose. Certification in anaplastology is provided by the Board for Certification in Clinical Anaplastology (BCCA), and requires studies in the arts and sciences. Specifically photography, illustration, sculpture, superficial anatomy, and polymer science are emphases of study. The authors’ institution has a facial prosthetics clinic staffed by a certified clinical anaplastologist (CCA) in which one can provide prostheses as an alternative to surgical reconstruction for total nasal defects. Patients with full-thickness complex nasal defects are referred by the senior author to the CCA in the Johns Hopkins Department of Art as Applied to Medicine for consultation. The CCA, in careful consultation with the patient and through use of predefect photographs, constructs a model of the patient’s original nose using wax ( Fig. 1 ). This model is approved by both the surgeon and the patient, and a duplicate is formed. At this point, the senior surgeon defines the subunits of the nose and the outer perimeter ( Fig. 2 ). The model is then sent to Direct Dimensions, Inc (Owings Mills, MD) for creation of the intraoperative surgical guide.

Creation of the translucent 3D intraoperative guide
Direct Dimensions, Inc
Direct Dimensions, Inc (DDI) has expertise in the application of geometric measurement technology. Employing techniques in data measurement, inspection, and reverse engineering, DDI can digitally “clone” a 3-dimensional product.
3D Data Acquisition
There are multiple ways to collect 3D data, but two of the most common methods are laser scanning and digitizing. During laser scanning, surface data are captured by a camera sensor mounted in the laser scanner recording accurate dense 3D points in space. This noncontact-based method of acquisition includes subtypes such as laser line, patch, and spherical. The surface laser scanner used for the authors’ nasal prostheses is from Perceptron Laser Scanning Systems (Plymouth, MI). The machinery for surface laser scanning costs approximately $80,000, and requires a year of training and experience to operate it effectively.
Digitizing involves contacting a probe on various points on the surface of the object to collect 3D information. Unlike laser scanning, which collects a large area of points at one time, digitizing allows one to record individual data points. This method is more accurate for defining the geometric form of an object rather than organic freeform shapes. Recently, photo-image–based systems are being used more frequently in 3D scanning.
3D Data Analysis
Digital modeling is the process of creating a computer model of an object that exactly replicates the form of the object. The surface laser scanner produces 3D point cloud data, and using PolyWorks software (Inovmetric Software, Inc, Quebec City, QC, Canada), a 3D polygonal model is created. A polygonal model is a faceted model consisting of many triangles formed by connecting the points within the cloud data. This software costs approximately $15,000, and requires 2 years of training and experience to operate effectively.
Rapid Prototyping
The digital 3D model is divided into vertical thirds and offset from the external surface contour. Because the intraoperative guide is only supposed to approximate the subsurface framework, there is reduction in height to accommodate for the eventual placement of the paramedian forehead flap. The top third is often left unaltered, the middle third is offset by 1 mm, and the bottom third is offset 1.5 to 2 mm. These parameters may be subject to change, given unique elements of the defect and individual variability in skin thickness. Once the surgeon and anaplastologist approve of the digital model, a rapid prototype is made of a semitransparent resin material. The machine that produces the rapid prototype retails for approximately $80,000, and requires 3 months of training and experience to operate effectively. During surgical reconstruction, to be discussed later, it has been found that it is easier to use a translucent guide as opposed to a semitransparent guide ( Fig. 3 ). To do this, a negative is made of the semitransparent mold and a 1.5 mm thick thermoforming clear baseplate is then vacuformed over the negative model. Trimming is done as necessary, and openings are made for the nostril. The template is sterilized for intraoperative use with cold sterilization (using iodine solution; STERRAD Sterilization Systems, Advanced Sterilization Products, Miami, FL). The overall cost for an individual nasal intraoperative guide is approximately $1100, broken down as follows: $250 for laser scanning, $650 for software analysis, and $250 for production of the rapid prototype.

Related posts:
 Foreword
Foreword
 3D and the Next Dimension for Facial Plastic Surgery
3D and the Next Dimension for Facial Plastic Surgery
 The Use of 3D Imaging Tools in Facial Plastic Surgery
3D Analysis of Tissue Expanders
Evolution of 3D Surface Imaging Systems in Facial Plastic Surgery
The Use of 3D Imaging Tools in Facial Plastic Surgery
3D Analysis of Tissue Expanders
Evolution of 3D Surface Imaging Systems in Facial Plastic Surgery
 3D Volume Assessment Techniques and Computer-Aided Design and Manufacturing for Preoperative Fabrication of Implants in Head and Neck Reconstruction
3D Volume Assessment Techniques and Computer-Aided Design and Manufacturing for Preoperative Fabrication of Implants in Head and Neck Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


