DOCK8 deficiency is an autosomal recessive combined immunodeficiency disease associated with elevated IgE, atopy, recurrent sinopulmonary and cutaneous viral infections, and malignancy. The DOCK8 protein is critical for cytoskeletal organization, and deficiency impairs dendritic cell transmigration, T-cell survival, and NK cell cytotoxicity. Early hematopoietic stem cell transplantation is gaining prominence as a definitive treatment given the potential for severe complications and mortality in this disease. Recently, DOCK2 deficiency has been identified in several patients with early-onset invasive bacterial and viral infections.
Key points
- •
DOCK8 deficiency is an autosomal recessive hyper–immunoglobulin E syndrome associated with atopy, recurrent sinopulmonary and cutaneous viral infections, and malignancies.
- •
The DOCK8 protein plays an important role in cytoskeletal organization, impacting dendritic cell transmigration.
- •
DOCK8 deficiency leads to persistence of B cells in germinal centers, early T-cell death, and lowered natural killler cell cytotoxicity.
- •
DOCK2 deficiency has been recently described in several patients with early-onset invasive bacterial and viral infections.
| Cdc42 | G protein activated by DOCK guanine exchange factors. |
| DOCK2 | Dedicator of cytokinesis 2, one of a class of guanine nucleotide exchange factors whose role is to activate the G protein Rac. |
| DOCK8 | Dedicator of cytokinesis 8, one of a class of guanine nucleotide exchange factors whose role is to activate G proteins such as Rac and Cdc42. Deficiency leads to impaired cytoskeletal organization and a phenotype of combined immunodeficiency with eczema, elevated IgE, and malignancy. |
| HSCT | Hematopoietic stem cell transplantation, a treatment for primary immunodeficiencies that result from genetic defects in hematopoietic cells. |
| ICAM-1 | Intercellular adhesion molecule 1, a ligand for LFA-1 necessary for leukocyte endothelial transmigration. |
| LFA-1 | Lymphocyte function–associated antigen 1, binds to ICAM-1 and functions as an adhesion molecule. |
| MST1 | Macrophage-stimulating 1 (also known as STK4). Deficiency results in a rare form of immunodeficiency with a phenotype similar to DOCK8 deficiency. |
| MyD88 | Myeloid differentiation primary response 88, a protein used by Toll-like receptors to activate the transcription factor NF-κB. |
| PGM3 | Phosphoglucomutase 3, which mediates glycosylation. Deficiency results in a phenotype of severe atopy, hypergammaglobulinemia, leukopenia, and developmental delay. |
| Rac | G protein activated by DOCK guanine exchange factors. |
| Rho GTPase | G protein such as Cdc42 and Rac, activated by DOCK guanine exchange factors. These proteins regulate various aspects of cytoskeletal dynamics. |
| STAT3 | Signal transducer and activator of transcription 3, a transcription factor. Deficiency leads to autosomal dominant hyper-IgE syndrome. |
| TLR9 | Toll-like receptor 9, important for activation of innate immunity via MyD88. |
| Tyk2 | Tyrosine kinase 2, a protein involved in IL-10 and IFN-α signaling. Deficiency has been associated with a variable phenotype that includes susceptibility to mycobacterial infection. |
| WAS | Wiskott-Aldrich syndrome is a rare X-linked recessive disease classically characterized by a triad of recurrent sinopulmonary infections, eczema, and thrombocytopenia with small platelets. Many patients do not exhibit the classic triad and may have autoimmune disease among other manifestations. |
| WASp | Wiskott-Aldrich syndrome protein, a protein that coordinates cytoskeletal reorganization. Deficiency leads to WAS. |
Introduction
Dedicator of cytokinesis 8 (DOCK8) deficiency is an autosomal recessive combined immunodeficiency syndrome characterized by recurrent sinopulmonary and cutaneous viral infections, as well as an increased immunoglobulin (Ig)E level and atopy. Although patients with an autosomal recessive variant of hyper-IgE syndrome had been described as early as 2004, a genetic basis involving bi-allelic mutations often with large deletions was not established until 2009. In the intervening years, definitive treatment with early hematopoietic stem cell transplantation (HSCT) has gained prominence, and advances have been made in understanding the functions of DOCK8 in dendritic cell and lymphocyte activity. Recently, another syndrome with differing phenotype but similar immunopathogenic basis, dedicator of cytokinesis 2 (DOCK2) deficiency, has been described.
Introduction
Dedicator of cytokinesis 8 (DOCK8) deficiency is an autosomal recessive combined immunodeficiency syndrome characterized by recurrent sinopulmonary and cutaneous viral infections, as well as an increased immunoglobulin (Ig)E level and atopy. Although patients with an autosomal recessive variant of hyper-IgE syndrome had been described as early as 2004, a genetic basis involving bi-allelic mutations often with large deletions was not established until 2009. In the intervening years, definitive treatment with early hematopoietic stem cell transplantation (HSCT) has gained prominence, and advances have been made in understanding the functions of DOCK8 in dendritic cell and lymphocyte activity. Recently, another syndrome with differing phenotype but similar immunopathogenic basis, dedicator of cytokinesis 2 (DOCK2) deficiency, has been described.
Clinical presentation of dedicator of cytokinesis 8 deficiency
Atopy
Patients with DOCK8 deficiency demonstrate atopy early on. Nearly all patients exhibit atopic dermatitis (AD), which ranges from mild to very severe and difficult to treat ( Fig. 1 ). Unlike patients with autosomal dominant hyper-IgE syndrome from Signal transducer and activator of transcription 3 (STAT3) mutations, many have food allergies with anaphylaxis, as well as asthma. Eosinophilic esophagitis also has been seen with increased frequency.
Infections
Cellulitis and skin abscesses are common, as is mucocutaneous candidiasis. There is a striking susceptibility to cutaneous infections by viruses, such as human papillomavirus (HPV) leading to widespread and recalcitrant warts, extensive and disfiguring molluscum contagiosum, herpes simplex virus (HSV) with recurrent or persistent lesions or herpes keratitis, and varicella zoster virus (VZV) with severe primary infection or recurrent zoster ( Fig. 2 ). Chronic Epstein-Barr virus (EBV) viremia is frequent, and may be associated with transformation to malignancy. Interestingly, severe systemic viral infections are less common, although several patients have suffered from cytomegalovirus (CMV) disease, encephalitis, and progressive multifocal leukoencephalopathy.
Most patients have a history of recurrent sinusitis and otitis media requiring tympanostomy tubes. Most also have had multiple pneumonias, with development of bronchiectasis in more than a third but infrequent pneumatocele formation ( Fig. 3 ).
Malignancy
Increased risk of neoplasms, especially hematological and epithelial, is an important feature of DOCK8 deficiency, and malignancy is often particularly aggressive and has early onset. In one large cohort of 136 patients, 17% of patients were diagnosed with malignancy at a median age of 12 years. Malignancy most frequently arises from poor control of viruses including squamous cell carcinomas from HPV infection and EBV-related lymphomas. Microcystic adnexal carcinoma, aggressive cutaneous T-cell lymphoma, and diffuse large B-cell lymphoma have been described. Of note, not all tumors have been associated with viral infection.
Other Clinical Manifestations
Vascular abnormalities have been recognized in more than 10% of patients in 2 recently described large cohorts ( Fig. 4 ). Cerebral aneurysms and stenosis are seen, and have been associated with stroke. Vaccine strain varicella was identified as the etiologic agent in one case, but in others an infectious has not been identified. Aortic aneurysm and abdominal arterial vasculitis also have been described, without known etiology. Autoimmunity rarely has manifested in other forms, such as hemolytic anemia. Liver disease, both associated with and without cryptosporidia has been described as well, and can be quite significant, leading to liver transplantation.
Laboratory Features
DOCK8 deficiency is a combined T-cell and B-cell immunodeficiency. In the initial cohort of patients described by Zhang and colleagues, all were noted to have normal neutrophils and monocytes. Ninety percent had low total T cells and CD8+ T cells, and all had low CD4+ T cells; 36% had low B and 60% low natural killer (NK) cells. In addition, there was poor CD8+ but not CD4+ T-cell proliferation in response to stimulation. Engelhardt and colleagues observed lower rates of T-cell lymphopenia in their 2009 and 2015 cohorts (38% and 27%, respectively), whereas Aydin and colleagues observed low total lymphocyte counts in 20% of patients but low total T cells and CD4+ T cells in nearly half of patients.
Elevated IgE and eosinophilia were nearly ubiquitous. Consistently, IgG levels were usually normal or elevated, IgA levels were variable, and IgM levels tended to be low and to decline with age. Vaccine responses to polysaccharide and protein antigens were variable, but the patients followed by Zhang and colleagues showed protective titers to rubella and VZV. Half of patients had low or absent specific antibody responses to pneumococcus, diphtheria, tetanus, or Candida . Memory B cells in patients with DOCK8 deficiency were near absent, as were switched memory B cells. Memory T-cell numbers were variable, but in one study most CD8+ cells had an exhausted CD45RA+/CCR7– phenotype. Caracciolo and colleagues noted low numbers of naïve and recent thymic emigrant T lymphocytes, along with Th2 skewing. This is consistent with low T-cell receptor excision circles in 3 children with DOCK8 deficiency, a finding with ramifications for potential early detection of this disease.
Making the Diagnosis
Given the potential for severe infection and malignancy, it is important to recognize DOCK8 deficiency before development of serious complications whenever possible. Diagnosis may be difficult, and, particularly in infants and young children, early presentation may significantly overlap with severe AD in both laboratory and clinical features. Genetic sequencing is key to making the diagnosis, but the expense makes this prohibitive for screening. Thus, several groups have sought to identify markers that can clue in the clinician to an underlying monogenetic disorder. Furthermore, distinguishing features of different monogenetic hyper-IgE syndromes on presentation is important for targeting subsequent evaluations.
When compared with patients with severe AD, patients with DOCK8 deficiency were more likely to have low total T cells, low CD4+ T cells, and decreased naïve CD8+ T cells in one small study. Total B lymphocyte numbers did not differ significantly between the 2 groups, but subsets revealed decreased memory and increased naïve and transitional B cells in the patients with DOCK8 deficiency.
When examining IgE-sensitization patterns in AD, STAT3 deficiency, and DOCK8 deficiency, Boos and colleagues found that patients with AD had the highest ratios of aeroallergen-specific IgE to total IgE, whereas patients with DOCK8 deficiency showed the highest serum-specific IgE against food antigens, followed by patients with AD.
Using the hyper-IgE syndrome scoring system developed by the National Institutes of Health, Engelhardt and colleagues compared clinical and laboratory scoring for DOCK8 and STAT3 patients and identified several objective features that were helpful in distinguishing the 2 syndromes: parenchymal lung abnormalities, retained primary teeth, and minor trauma fractures were deemed most consistent with STAT3 deficiency. Characteristic facies was also significantly associated with STAT3 deficiency but was considered a subjective assessment. By assigning negative points to the 3 features and adding points based on absolute eosinophil count and frequency of sinus and ear infections, the group developed a DOCK8 score that appears promising but has yet to be validated.
Another study featured long-term follow-up of biomarker trends in individual patients with DOCK8 deficiency and STAT3 deficiency. Patients with DOCK8 deficiency demonstrated consistently lower total, CD4+, and CD8+ T-cell numbers but normal Th17 cells as opposed to low Th17 cell but otherwise normal numbers of T cells in patients with STAT3 deficiency. In terms of clinical characteristics, the investigators suggested that a history of recurrent viral infections, bronchial hyperreactivity, food allergies, and consanguinity should prompt greater concern for DOCK8 deficiency.
In addition to severe AD and STAT3 deficiency, the differential diagnosis for a patient with AD, elevated IgE, and recurrent infections includes several other genetic disorders.
- •
Wiskott-Aldrich syndrome (WAS) is characterized by T-cell lymphopenia, poor lymphocyte proliferation, impaired NK cytotoxicity, autoimmunity, and malignancy. The WAS protein (WASp) coordinates cytoskeletal reorganization downstream from DOCK8, which accounts for some overlap in phenotype, including recurrent bacterial and viral infections, eczema, and vascular abnormalities. Distinguishing features of WAS include X-linked inheritance and microthrombocytopenia.
- •
Phosphoglucomutase 3 (PGM3) deficiency, a congenital disorder of glycosylation, has been recently identified in patients who, in addition to severe atopy and hypergammaglobulinemia, usually have lymphopenia and neutropenia. Developmental delay or neurologic impairment is common.
- •
Omenn syndrome is a form of severe combined immunodeficiency associated with several different genetic defects. Severe erythroderma and exfoliative dermatitis are evident in early infancy, along with elevated IgE, infections, lymphadenopathy, and hepatosplenomegaly.
- •
STK4 or Macrophage-Stimulating 1 (MST1) deficiency, discovered within the past few years, has a phenotype similar to DOCK8 deficiency, with cutaneous viral, bacterial, and fungal infections, recurrent respiratory infections, and CD4 lymphopenia. AD seems to be milder, and IgG and IgA are elevated as well as IgE. Cardiac anomalies have been noted in multiple patients.
- •
Tyk2 deficiency was described in 2006 in a patient with elevated IgE, AD, recurrent skin staphylococcal abscesses, and mycobacterial infection. However, recently, 7 new patients with Tyk2 deficiency were identified, all with normal IgE, calling into question the classification of Tyk2 deficiency as a hyper-IgE syndrome.
Related posts:
 Basic Science Insights into Clinical Puzzles
Basic Science Insights into Clinical Puzzles
 Establishing Tolerance to Commensal Skin Bacteria
Understanding Inherited Cylindromas
Establishing Tolerance to Commensal Skin Bacteria
Understanding Inherited Cylindromas
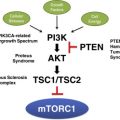 Mosaic Disorders of the PI3K/PTEN/AKT/TSC/mTORC1 Signaling Pathway
Interleukin-22 and Cyclosporine in Aggressive Cutaneous Squamous Cell Carcinoma
Mosaic Disorders of the PI3K/PTEN/AKT/TSC/mTORC1 Signaling Pathway
Interleukin-22 and Cyclosporine in Aggressive Cutaneous Squamous Cell Carcinoma
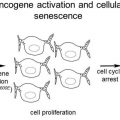 Melanocytic Nevi and the Genetic and Epigenetic Control of Oncogene-Induced Senescence
Melanocytic Nevi and the Genetic and Epigenetic Control of Oncogene-Induced Senescence
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


