Although restoration of hand function in brachial plexus patients remains a formidable challenge, the past decade has brought significant improvement in our ability to restore hand function even in the most severe cases. Today, the following options are available to restore hand function: (1) direct nerve repair; (2) nerve grafting; (3) nerve transfers from intraplexal or extraplexal sources; (4) tendon transfers (and tenodesis); (5) free functioning muscle transfer; (6) arthrodesis; and (7) a combination of these techniques. Opportunity for future improvement exists, and the next decade will no doubt bring further innovation.
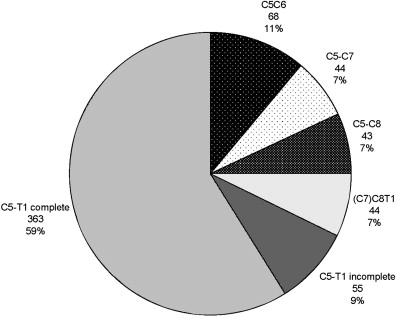
Brachial plexus injuries are devastating, and are associated with high levels of disability and decreased health status. The hand is affected in the vast majority of injuries ( Fig. 1 ). Over the past decade, innovative applications of nerve transfers and free functioning muscle transfers (FFMT) have offered patients, particularly those with pan-plexus injuries, hope of regaining some hand function. Nevertheless, restoration of hand function in adult brachial plexus patients remains a formidable reconstructive challenge.
Several recent reviews describe the management and treatment of adult brachial plexus lesions. The current status of nerve transfers, tendon transfers, and FFMT are reviewed in articles elsewhere in this issue. The purpose of this article is to focus on the reconstructive options available for the restoration of hand function (ie, prehension) in adult brachial plexus patients.
Motor and sensory deficits in the hand following brachial plexus injury
The root contribution to each upper extremity muscle is variable. In addition, a prefixed or postfixed brachial plexus can further confound clinical expression of a root lesion. Following a stretch injury, each nerve fiber in the root, trunk, or peripheral nerve sustains a unique histologic lesion (ie, Sunderland 1–5) such that one portion of a root may recover spontaneously and another portion may not. These factors contribute to significant variability in the expression of motor or sensory deficits following a root lesion(s). Each clinical case is unique and a detailed clinical examination is always required. Clinicians broadly group brachial plexus lesions into upper (C5C6) or lower (C8T1) plexus lesions with or without involvement of C7 ( Table 1 ).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


