○ Xenon flashlamp (light source) emits noncollimated, noncoherent, and polychromatic light (broad wavelength range: 500–1200 nm)
○ A variety of filters are utilized to narrow down the range of wavelengths to target the same chromophores that lasers do
○ Less selective and less powerful than lasers
○ Electrodes deliver alternating electric current ➔ locally heats tissue
○ Much less selective and less powerful than lasers and IPL, but does have some specificity for fat (hence, RF is used primarily for cellulite, and to a lesser extent, skin tightening)
Laser safety
• Four main concerns: blindness, fire hazards, cutaneous burns, and inhalation of biohazardous plume
■ Up to 7% of emitted laser light is reflected by the stratum corneum ➔ reflected light can cause eye damage/blindness (may occur if even 1% of the beam is reflected into eye)
■ Blindness is rapid and painless
■ Any laser/light source in UV range ➔ lens damage, cataracts
○ Example: excimer laser (308 nm)
■ Any laser/light source that targets melanin or hemoglobin (visible light and near-infrared wavelengths) ➔ retinal damage (retina is highly pigmented); also damages uvea and iris
○ Examples: KTP (532 nm), PDL (585–600 nm), ruby (694 nm), IPL (various wavelengths), alexandrite (755 nm), diode (800 nm), and Nd:YAG (532 nm and 1064 nm)
○ Highest risk = near infrared and Q-switched lasers
■ Any laser/light source that targets water (mid and far-infrared wavelengths) ➔ corneal/scleral damage
○ Examples: Nd:YAG (1320 nm), Erbium:glass (1550 nm), Erbium:YAG (2940 nm), and CO2 (10 600 nm)
■ Greatest fire risk with CO2 and Erbium:YAG ablative and fractionated lasers
■ Risks: drapes, clothing, dry hair, and plastic tubes (endotracheal tubes, especially if oxygen is being administered)
■ Prevention: moisten hair near treatment field, ensure that any alcohol/acetone skin cleanser has fully dried before using laser, and reduce intraoperative O2 concentration <40%
• Cutaneous burns: may occur with any laser or nonlaser energy source (IPL and RF); as a result of operator error
• Inhalation of biohazardous plume
■ HPV viral particles have been detected in laser plumes ➔ cases of laser-surgeons developing HPV-16-induced oral SCC related to inhalation
■ Prevention: ventilation and/or smoke evacuator; also recommend N95 mask
Vascular lasers
• Commonly treated vascular lesions: blood vessels as a result of photoaging, redness associated with (a/w) rosacea, spider angiomas, Poikiloderma of Civatte, hemangiomas, vascular malformations, redness in striae, redness in scars, verruca vulgaris, and Kaposi sarcoma (less common)
• Utilize selective photothermolysis to damage blood vessels via coagulation of vessel contents ➔ vessel collapse or destruction
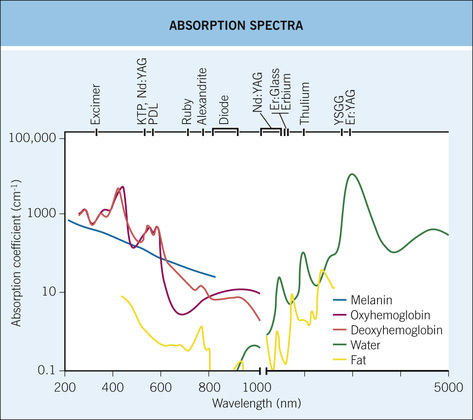
• Target: hemoglobins (oxyhemoglobin > deoxyhemoglobin > methemoglobin)
■ Absorption peaks = 418, 542, and 577 nm
• Main SE = purpura (primarily PDL)
■ Other SEs dyschromia (↑risk in darker skinned patients), blistering (↑risk with shorter pulse widths, higher fluences, and skin of color)
• Skin cooling via precooling is critical ➔ prevents epidermal damage
■ Also allows for greater patient comfort and allows physician to treat at higher, more efficacious fluences
• General anesthesia is recommended for larger pediatric lesions
• Consider HSV prophylaxis for perioral lesions, or larger facial malformations
• Desired treatment endpoints:
■ PDL – purpura (as a result of cavitation and vessel rupture)
○ Nonpurpuric regimens utilize pulse durations of 20 ms or higher ➔ do not get cavitation or vessel rupture ➔ do not get immediate purpura (but frequently get delayed purpura days later)
■ KTP, Nd:YAG – immediate disappearance of vessel
• Complex vascular lesions typically require several treatments
■ PDL (585–600 nm) is the treatment of choice for most vascular lesions (PWS, telangiectasias, erythematous scars, and hemangiomas)
■ IPL is the TOC for Poikiloderma of Civatte (treats both the vessels and dyschromia)
○ If IPL is not an option on the examination, PDL would be second best choice
■ Long-pulsed Nd:YAG (1064 nm) is the laser of choice for most vascular ectasias on the lower leg (venulectasias, telangiectasias, and reticular veins), because it penetrates deeper than other vascular lasers
○ Diode (800 nm) would be the second best choice
■ IPL or long-pulsed PDL (nonpurpuric) are the treatments of choice for erythematotelangiectatic rosacea
Hair reduction lasers and light sources
• Common laser hair reduction uses: removal of unwanted hair, pseudofolliculitis barbae, hidradenitis suppurativa, and pilonidal cyst disease
• Laser hair reduction is based upon the principle of selective photothermolysis
• Target: melanin within hair shaft, ORS, and matrix
■ Absorption peaks: broad range (~300–1000 nm)
• Destruction of bulge and bulbar stem cells ➔ improved hair removal
• Dark, thick terminal anagen hairs respond best
■ Thinner, lighter hair is hard to remove
■ White hair is impossible to remove (lacks target chromophore) ➔ other epilation techniques recommended
○ Recommendation: treat test spot and follow up in 1 to 2 weeks
■ Blistering/burning (↑risk in skin of color) may ➔ scarring
• Requires multiple treatment sessions, spaced 4 to 6 weeks apart; treatments often not permanent ➔ goal is “reduction, rather than removal”
• Recommend shaving before treatment in order to shorten hairs ➔ ↓skin burns from hairs on skin surface
• Do NOT fully remove hair shafts by chemicals, waxing, plucking, or threading for at least 6 weeks before treatment (eliminates target chromophore)
• Desired treatment endpoint = transient perifollicular edema
• Use wavelength-specific eyewear to protect retina
• Use parallel cooling to protect the epidermis during treatment
■ Diode is most efficacious; usually safe in skin of color (but not as safe as Nd:YAG)
■ Nd:YAG (1064 nm) = safest hair removal laser in skin of color, but slightly less effective (Table 9-3)
Resurfacing lasers (Table 9-4)
• Common indications: rhytids, photoaging and actinic damage, acne scars, keloid, hypertrophic and burn scars, postsurgical scars, benign skin lesions (SKs/warts/syringomas), striae, and rhinophyma
■ Absorption peaks: 1450, 1950, and 3000 nm
• May be ablative or nonablative
■ Ablative lasers function by removing skin via vaporization of target tissue
■ Nonablative lasers work via subtle thermal effects on dermis ➔ stimulates a wound healing response
• May be fractionated or nonfractionated
■ Fractionated: creates thousands of microscopic thermal zones of injury (MTZ) ➔ stimulates turnover/remodeling of epidermis and dermis
○ Advantages: ↓downtime and ↓duration of erythema compared with nonfractionated resurfacing
○ Disadvantages: less efficacious; requires more treatment sessions
• Site of eye damage: cornea, sclera (burns)
• Consider HSV/fungal/bacterial prophylaxis
■ Erythema (often persists for months)
■ Relative hypopigmentation (↑risk if deeper injury; may arise months after treatment)
○ HSV: highest risk in first week
○ Bacteria (S. aureus, Pseudomonas)
Table 9-4
Resurfacing Lasers
| Laser | Wavelength | Comments |
| Ablative | ||
| Erbium:yttrium scandium gallium garnet (Er:YSGG) | 2790 nm | Less thermal injury ➔ poor coagulation, ↑bleeding, and ↓collagen retraction |
| Erbium:yttrium aluminum garnet (Er:YAG) | 2940 nm | Less thermal injury ➔ poor coagulation, ↑bleeding, and ↓collagen retraction Targets the 3000 nm absorption peak of water more effectively than CO2 laser Advantages compared with CO2 laser: ↓recovery time, ↓PIH, and erythema resolves more quickly |
| Carbon dioxide (CO2) | 10,600 nm | More thermal injury ➔ good coagulation, minimal to no bleeding, and ↑collagen retraction Depth of ablation is increased by performing more passes |
| Nonablative | ||
| Vascular lasers (PDL) | 585–600 nm | PDL +/− amino-levulinic acid: may also help treat coexisting AKs and actinic cheilitis |
| Infrared lasers | Nd:YAG (1064, 1320 nm) Diode (1450, 1470 nm) Er:glass (1540 nm) | All achieve mild dermal tightening, but do not help with epidermal sun damage Diode is more effective at treating acne scarring than others |
| IPL | 515–1200 nm | Leads to mild dermal tightening and also treats epidermal photodamage |
| Radiofrequency | NA | Electrical current heats dermis ➔ mild skin tightening |
Tattoo removal lasers (Table 9-5)
• Tattoo pigments are very small in diameter ➔ very short TRT (nanoseconds) ➔ QS-lasers are required
• Immediate tattoo whitening (desired endpoint) is a result of cavitation
• Amateur tattoos and black tattoos are the most responsive to treatment (usually <5 treatment sessions)
• Professional tattoos and multicolored tattoos most difficult to treat (>10 treatment sessions)
■ Mnemonic: “The 3 B’s (black, brown blue tattoos) RAN away when they saw the 3 lasers” ➔ all 3 colors are treated with Ruby, Alexandrite, or Nd:YAG
■ Mnemonic: “If you have a Yellow, White, Red, or Violet tattoo, You Will Return Visit for 2 or more treatments with frequency-(2)doubled Nd:YAG”
■ Only ruby and alexandrite treat green tattoos
■ Red tattoos (cinnabar [mercuric sulfide]) ➔ most likely to cause allergic reactions
■ Laser treatment in patient allergic to tattoo dye ➔ possible anaphylaxis
■ White tattoos may undergo immediate paradoxical darkening (turns black or blue) with laser because of reduction of Ti4+➔Ti3+
■ Pink, flesh-toned, or light red tattoos (classically, permanent lip liner) may undergo immediate paradoxical darkening (turns brown-black) with laser because of reduction of ferric oxide (Fe3+) ➔ ferrous oxide (Fe2+)
■ Traumatic tattoos from gunpowder/fireworks ➔ may explode with laser
■ Pigmented lesions (lentigines, ephelides, or nevus of Ota) are treated with the same lasers as black tattoos (“RAN” lasers)
○ Ruby is classically the laser of choice for nevus of Ota/Ito
■ Minocycline hyperpigmentation ➔ treated with the same lasers as black tattoos (“RAN” lasers)
Table 9-5
Tattoo Removal Lasers
| Tattoo Color | Pigment | Laser (All are Q-switched) | Wavelength (nm) |
| Black | Iron oxide, carbon, india ink, lead, and gunpowder | Ruby | 694 |
| Alexandrite | 755 | ||
| Nd:YAG | 1064 | ||
| Blue | Cobalt | Ruby | 694 |
| Alexandrite | 755 | ||
| Nd:YAG | 1064 | ||
| Brown | Ochre | Ruby | 694 |
| Alexandrite | 755 | ||
| Nd:YAG (frequency-doubled) | 532 | ||
| Nd:YAG | 1064 | ||
| Green | Chromium oxide, malachite green | Ruby | 694 |
| Alexandrite | 755 | ||
| Yellow | Cadmium sulfide, ochre | Nd:YAG (frequency-doubled) | 532 |
| White | Titanium dioxide, zinc oxide | Nd:YAG (frequency-doubled) | 532 |
| Red | Mercuric Sulfide (cinnabar), azo dyes, cadmium selenide, and sienna | Nd:YAG (frequency-doubled) | 532 |
| Violet | Manganese violet | Nd:YAG (frequency-doubled) | 532 |
9.2 Botulinum toxin
• Botulinum toxin is a neurotoxin derived from the anaerobic gram(+) bacilli Clostridium botulinum
• There are eight subtypes of botulinum toxin (A-H) (Table 9-6), but only two (types A and B) are in clinical use
Table 9-6
Botulinum Toxin Subforms and Site of Action
| Botulinum Toxin Subtype | Site of Action in SNARE Complex of Proteins |
| A | Snap-25 |
| B | SynaptoBrevin |
| C | Snap-25, Syntaxin |
| D | Synaptobrevin |
| E | Snap-25 |
| F | Synaptobrevin |
| G | Synaptobrevin |
| H | Synaptobrevin |
• Mechanism: Botulinum toxin inhibits the function of nerve terminals through presynaptic blockade of SNARE complex ➔ prevents acetylcholine (Ach) release ➔ chemical denervation of muscle ➔ over time, the muscle undergoes atrophy (Fig. 9-3)
• FDA-approved for the temporary improvement in the appearance of glabellar lines and the lateral canthi lines, as well as axillary hyperhidrosis
■ Effect typically lasts about 3 months, and may take up to 1 week to demonstrate full effect
■ Remember, rhytides are perpendicular to muscle fibers
• Three forms of botulinum toxin type A and one form of botulinum toxin B currently marketed in the USA (Table 9-7)
Table 9-7
Different Forms of Botulinum Toxin Type A in the United States
| OnabotulinumtoxinA | AbobotulinumtoxinA | IncobotulinumtoxinA | RimabotulinumtoxinB | |
| Brand name | Botox® | Dysport® | Xeomin® | Myobloc® |
| Molecular composition | 150 kDa neurotoxin with complexing proteins | 150 kDa neurotoxin with complexing proteins | 150 kDa neurotoxin | 150 kDa neurotoxin |
| Molecular weight | 900 kDa | 500–900 kDa | 150 kDa | 700 kDa |
| Recommended dose for glabellar lines | 20 U | 50 U | 20 U | 20 U |
| Target protein | Snap-25 | Snap-25 | Snap-25 | Synaptobrevin |
| Storage before/after reconstitution | 2–8°C/2–8°C | 2–8°C/2–8°C | <25°C/2–8°C | 2–8°C/2–8°C |
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


