CHAPTER 39 Correction of Breast Asymmetry in Teenagers
Summary and Key Points
Introduction
Correction of breast asymmetry in the adolescent girl is a challenging problem, and the treatment alternatives are numerous. The origin of the asymmetry may involve the development of the breast tissue itself, the foundation onto which the breast tissue rests, the invasion of the breast by anomalous lesions, or the deformation of the developing breast by surrounding tissue restriction.1
Indications
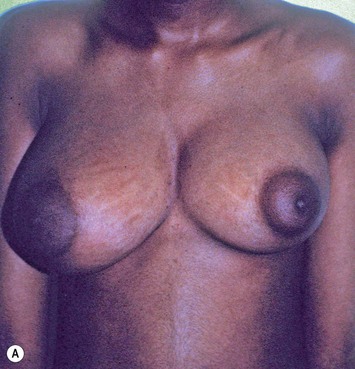
Developmental non-syndromic breast asymmetry may by reflected in either difference in size or difference in shape. Teenagers often present with overdevelopment of one breast and relative hypoplasia of the other, creating a mild to moderate asymmetry. A discussion must be undertaken to decide which breast volume the patient prefers. With mild to moderate asymmetries, it is often easiest to reduce the larger breast. Despite this, perfect symmetry remains a challenge, as only one breast is operated on. Augmentation of the smaller breast creates even more decision possibilities and symmetry challenges. The choice of material with which to augment must be selected: implant versus autologous. A unilateral implant offers an easy solution, but makes upper and lower pole symmetry with the opposite breast difficult, while autologous tissue involves more extensive surgery and donor site morbidity, albeit a more stable long term solution. Either of the latter options may still warrant contralateral breast surgery (i.e. mastopexy, reduction or augmentation) to achieve best symmetry. In the case of severe hypoplasia of the smaller breast, one has no choice but to augment the hypoplastic side, and the same decision making choices apply regarding which material to use. Additionally in this case, the possibility of increasing the skin envelope with prior expansion to obtain better ptosis must be contemplated. The treatment options are pushed yet further in the case of syndromic developmental breast asymmetry such as Poland’s syndrome. In Poland’s syndrome, variable unilateral hypoplasia, potential thoracic rib deformity along with variable absence of the pectoralis major muscle leads to all the above treatment alternatives to which is added a possible muscle transposition to correct the asymmetry (Fig. 39.1).

The thoracic cage is the foundation onto which the breast tissue rests. Asymmetry in the thoracic cage will secondarily translate into asymmetrically appearing breasts (Fig. 39.2). This is often seen in patients with scoliosis.2 Assessment of the scoliosis and resulting chest wall deformity must be recognized and related to the patient so that proper treatment options can be considered.

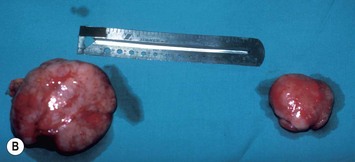
Breast asymmetry secondary to proliferation of anomalous lesions is relatively frequent, and proper examination is necessary to identify these lesions. Benign fibroadenomas are common lesions presenting in breast tissue, unilaterally or bilaterally (Fig. 39.3).3 These tumours are well circumscribed and can usually be removed completely. Preoperative ultrasonography is used to confirm the presence and location of the mass within the breast tissue.
Isolated Breast Asymmetry Reconstruction
With isolated breast asymmetry, multiple options are available depending on the severity of the asymmetry and the patient’s desires.4 With mild to moderate asymmetry one can decide to reduce the larger breast, or augment the smaller one.
Reduction of the larger breast is often the easiest solution if the contralateral breast is of sufficient volume and pleasing to the patient (Fig. 39.4). Despite this, perfect symmetry may still be problematic as only one breast is operated on, and symmetric degree of ptosis is more difficult to achieve. A contralateral mastopexy may help achieve a balanced result (Fig. 39.5).




Augmentation of the smaller breast may be the decided option. The use of an implant for augmentation allows for a simple way to augment breast volume and fill out upper and lower poles of the breast (Fig. 39.6). The lack of plasticity of an implant, however, makes it difficult to achieve ideal symmetry in breast shape and contralateral surgery is often indicated (Fig. 39.7). Upper pole fullness and a relative lack of natural ptosis tend to remain with this treatment option. Additionally, the potential for capsular contracture and need to eventual implant replacement in the long term is not negligible, particularly in teenagers.




The use of autologous material for augmentation obviates many of the problems that implants pose. The tissue not only responds to physiologic changes of weight gain, ageing, or hormonal variations, but additionally responds to gravitational forces creating a far more natural ptosis mimicking the opposite breast (Figs 39.8 and 39.9). Capsular contracture or other potential surgical procedures are no longer an issue with this treatment option. The choices of autologous tissues are multiple5–7 depending on the amount required and level of surgeon’s expertise. Microsurgical free tissue autologous reconstruction is technically more demanding and creates a donor site with resultant additional scars. The long term benefits, however, are still weighted favourably. The choice of free tissue transfer is dependent on patient physiognomy and surgeon’s experience. The adolescent patient often has little abdominal fat, so that a DIEP is often inadequate in volume. An SGAP or IGAP flap offers enough volume for the most part.5,8 The latter has become our preferred free tissue transfer option as the scar location is most appealing in the North American setting. When a relatively small amount of autologous tissue is required for augmentation, the use of a pedicled latissimus myocutaneous transfer may be a valid option. This circumvents the need for microsurgical technique. This latter option can be combined with a further augmentation procedure, either allogenic or autologous. Having said this, in some patients, even though autogenous reconstruction may seem the best option from the surgeon’s point of view, a prosthetic augmentation can be done early: it is a simpler procedure that does not compromise a later autologous transfer and may help the patient mature a few years.









Technical details of the inferior gluteal perforator flap harvest
Mapping of the perforators is done prior to surgery with the patient in lateral decubitus position using a color Doppler to locate the major perforators as they exit the muscular aponeurosis (Fig. 39.10






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


