CHAPTER 24 Coronal browlift
Physical evaluation
• Attain a thorough ocular and eyelid history, past medical history, past facial surgical history, craniotomy scars, and forehead trauma.
• Check the visual acuity of each eye.
• Examine the brow position relative to the anterior hairline as well as superior orbital rim.
• Brow ptosis and upper lid skin.
• Skin quality and rhytid depth in the medial and lateral forehead.
• Document the motor and sensory function to the forehead.
• Examine the scalp hair quality and follicle density.
Anatomy
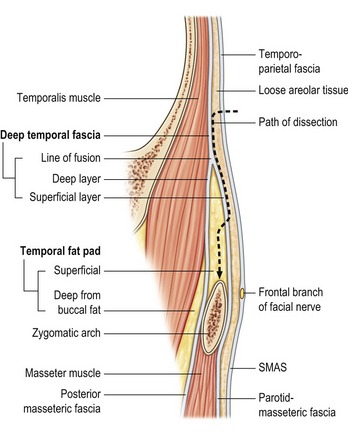
Understanding the temporal and forehead anatomy is critical to successful browlift surgery (Fig. 24.1). The scalp is composed of five layers (Skin, Connective tissue, galea Aponeurotica, Loose areolar connective tissue, and Periosteum). The blood supply to the forehead scalp is from the internal (supratrochlear, supraorbital) and external carotid (superficial temporal) arteries. Hair follicles are located in the subcutaneous layer. Injury to the follicles results in temporary or permanent alopecia. The frontal branch of the facial nerve is located in the superficial temporal fascia and innervates the muscles of the forehead (frontalis, corrugators, depressor supercilii, and procerus). The supratrochlear and supraorbital nerves provides sensation to the central and lateral forehead as well as portions of the anterior scalp.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


