Abstract
Patients with neuromuscular diseases, such as myasthenia gravis, must be warned that botulinum toxin could potentiate their weakness. Some drugs, such as aminoglycosides and anaesthetic agents, will interfere with the effect of botulinum toxin and could result in an overdose. Other drugs, such as antimalarials and cyclosporin, may reduce the effect of the treatment and also the duration. Patient expectations must be informed and realistic. Examine carefully to anticipate an asymmetric response, and advise patients to return for a check-up within 3 weeks. They often benefit from a ‘balancing treatment’. Warn the patient if he or she is likely to bruise due to medications or medical history. Most complaints can be avoided by selecting the correct site of treatment and dose for the patients. Recommend surgery first if they have ptosis or preexisting blepharochalasis or brow sagging and want to cease overarching their eyebrows. Very rarely, patient can develop antibodies to botulinum toxin, reducing the effect. A trial with a different serotype may be rewarding instead.
Keywords
Myasthenia Gravis, Botox, Dysport, Azzalure, paralysis, antibodies, ptosis, symmetry
The right way to select patients for treatment with botulinum toxin (BTX) is described in detail in Chapter 6 , and some well-established contraindications must always be kept in mind.
Absolute contraindications
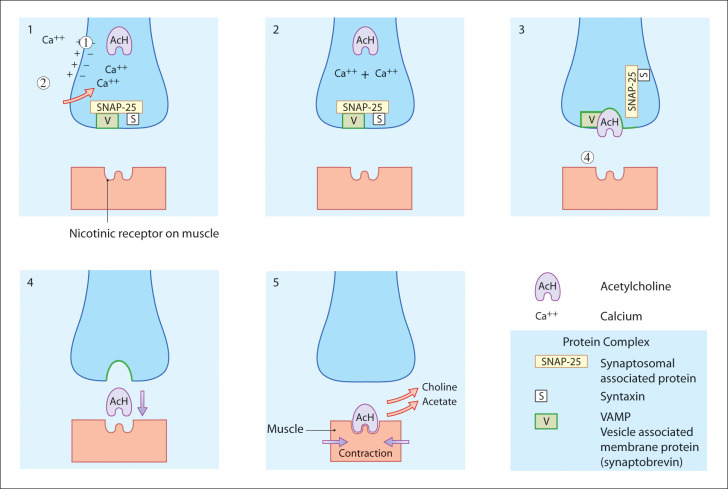
Anything that interferes with the predicted response to BTX, which inhibits the release of acetylcholine at the neuromuscular synapse ( Fig. 7.1 ).
- a.
Drugs and disorders which also reduce acetylcholine at the motor end plate, amplifying the action of BTX:
- ■
Eaton-Lambert antibodies. Note a history of cancer, metastases and general lack of well-being which may suggest a diagnosis of Eaton-Lambert syndrome (see ‘Neuromuscular Disorders’).
- ■
Aminoglycosides (gentamycin, streptomycin, kanamycin) act on the presynaptic neurone.
- ■
- b.
Drugs and disorders which alter the response of the motor end plate, amplifying the action of BTX:
- ■
Myasthenia gravis alters and reduces the acetylcholine receptors on the motor end plate (see section on ‘Neuromuscular Disorders’).
- ■
Medication with succinylcholine (an agonist blocker) produces a prolonged depolarisation with reduced contraction.
- ■
Tubocurare, pancuronium and gallamine are antagonist blockers that compete with acetylcholine for end-plate receptor sites.
- ■
D-penicillamine can produce myasthenia gravis–type antibodies.
- ■

Drugs which reduce the action of BTX
The antimalarials chloroquine and hydroxychloroquine, and the immunosuppressant cyclosporin, can reduce the action of BTX.
Neuromuscular disorders
It is of paramount importance to avoid BTX in patients with neuromuscular disorders. Many such disorders are inherited and so a thorough family history must be taken with this point in mind.
General and local anaesthesia
Administering BTX at the time of general or local anaesthesia gives less predictable results. Avoid injecting BTX to the eye zone in patients who have had local anaesthesia for blepharoplasty.
Also avoid giving BTX in the postoperative phase where there is local oedema, to reduce the risk of distal diffusion and, for example, perioral palsy.
Contraindications:
Eaton-Lambert syndrome
Myasthenia gravis
Neuromuscular disorders (check family history).
Aminoglycosides (streptomycin, gentamycin, kanamycin)
Certain drugs used during anaesthesia (e.g. succinylcholine, tubocurare)
d-Penicillamine—used in rheumatoid arthritis
Chloroquine, hydroxychloroquine (antimalarials)
Cyclosporin (immunosuppressant)
Pregnancy
Infection
Pregnancy and breastfeeding
The teratogenicity of BTX has not yet been established and so it is contraindicated in pregnancy and during breastfeeding. There are reports in the literature of dozens of women who inadvertently received BTX whilst unknowingly pregnant. One percent miscarried, and there appears to be no obvious association.
Allergy
A history of allergy to any ingredient in the formulation, including albumin. Reports of allergic reactions include local rashes. For noncosmetic patients requiring BTX (e.g. with cervical dystonia), IncaBTX-A (Xeomin), with its lower protein load, may prove a safe alternative but must be used judiciously.
Search the patient’s history for any hint of muscle or nerve weakness that he or she may not be aware of. Enquire about episodes of intermittent drooping of the eyelid.
Take care to document that the patient has denied any contraindications.
Relative contraindications
Many patients who come for BTX treatment for rhytids are self-referred. Their motivation is based either on a drive for self-improvement or a desire to ‘have what their friend has had’, that is a wrinkle-free forehead. Reserve judgement on their suitability for treatment until a careful assessment has been carried out. This is dealt with in detail in Chapter 6 , and most of the side effects discussed can be avoided by rigorous patient selection. In addition, patients must be provided with detailed written information about the poisonous nature of BTX and the other risks associated with treatment.
If fully informed, most patients have reasonable expectations. Once in possession of all the facts, they are in a position to decide what risks to take and when. They may be happy to risk walking down the aisle with a camouflaged bruise or may prefer to postpone this risk until after their ‘big day’ and opt to keep their frown instead. If their treatment will be unpredictable (e.g. the treatment of a deep frown in a patient with moderate lash/brow distance and a moderate transient risk of immobile brows), then let them know about this. They can always change the date of their appointment to avoid it clashing with a big occasion.
Avoid treating patients who cannot fully understand the risks being discussed.
Table 7.1 lists the most frequent complaints encountered in the author’s practice during more than 30 years of treatments with BTX for rhytids. During this time, the incidence of complaints has dropped dramatically, probably as a result of more rigorous patient selection and counselling, but also generalised public awareness.
| Complaint | Most Likely Cause |
|---|---|
| It didn’t work! | BTX denatured. |
| It didn’t last! | BTX too dilute or too old. |
| I’m still frowning! | Patients do not understand what you have told them about their low brows and the treatment of frown! (see Chapter 9 ) |
| Patient looks tired | BTX to forehead causes brow ptosis. |
| My eyes are swollen! | Due to protrusion of upper and lower lid orbital fat and skin from weight of flaccid brows and flaccid lower septum. |
| Hollow socket | BTX to inferolateral canthus in certain patients. |
| Peaked eyebrows | BTX over 75% of medial brow only. |
| Epiphora | BTX over lacrimal pump. |
| Severe bruising | BTX over branch of maxillary vein. |
| Unnaturally wide palpebral aperture | BTX to pretarsal orbicularis muscle. |
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


