This article aims to provide an update on techniques related to head and neck reconstruction using microvascular free tissue transfer, focusing on strategies for donor vessel selection in the vessel depleted neck, use of vein grafting and mechanical arterial coupling, estimating flap volume loss, and utilization of virtual planning and medical modeling for midface and mandibular reconstruction.
Key points
- •
Many nontraditional cervical and non-cervical vessels have been used with success for anastomosis in posttreatment necks with limited vessels.
- •
Vein grafting allows for increased pedicle lengths when required for successful anastomosis.
- •
Although rare, mechanical coupling has been used successfully for arterial anastomosis, mostly in salvage surgical settings.
- •
It is difficult to accurately estimate flap volume loss postoperatively and further studies are warranted.
- •
Virtual planning and medical modeling is a useful and cost-effective tool for midface and mandibular reconstruction.
Introduction
Microvascular free tissue transfer, commonly referred to as “free flap” procedures, is a hallmark of reconstruction of complex head and neck defects following ablation of both benign and neoplastic processes. Here were present an update on head and neck reconstruction, including strategies for managing a vessel depleted neck, considerations in vein grafting, the potential indications and use of mechanical couplers for arterial anastomosis, accounting for free flap tissue loss postoperatively, and the use of virtual planning and medical modeling.
Vessel depleted neck
Previous treatment in the form of surgery, radiation, or both can lead to challenges in revision free flap surgery. Prior surgery and radiation lead to disruption of tissue planes and scarring, which can increase risk of damage to vessels and make identification of viable recipient vessels difficult. , A recent multi-institutional study highlighted the added challenges of reconstruction after both radiation and a prior ipsilateral free flap. Hanasono and colleagues examined over 200 patients who required microvascular free tissue transfer following either neck dissection and/or cervical radiation and found almost 20% of patients did not have suitable ipsilateral external carotid branches for anastomosis. The same group later examined arterial vessels used across 273 microvascular free tissue transfer procedures, noting that while the ipsilateral facial artery was the most commonly used recipient vessel for initial surgery, second and third procedures most frequently used either the ipsilateral superior thyroid or contralateral facial arteries. Chang and colleagues found that facial artery and vein were significantly less likely to be used when an ipsilateral microvascular free tissue transfer had previously been performed. Both studies also highlight the utility of arterial anastomosis directly to the external carotid artery as a viable option when ipsilateral cervical vessel options are limited. ,
Options for recipient vessels beyond unused cervical vessels include vessels outside the prior radiation of surgical fields. The subclavian artery lies in the inferior neck and provides alternative cervical anastomotic options. The first branch of the subclavian artery is the vertebral artery, and to our knowledge this has not been utilized in free flap reconstruction, almost certainly due to risk of neurologic ischemia. The internal mammary artery branches inferiorly from the subclavian artery and descend into the thoracic cavity. Use of this artery will be discussed later in this section. The next major branch of the subclavian artery is the thyrocervical trunk, which has 2 branches that are frequently used for arterial anastomosis: the transverse cervical and supraclavicular arteries. The transverse cervical artery lies immediately deep to the fascia that serves as the deep boundary of level 4 neck dissection and thus is frequently seen, but not dissected in previous surgeries. In our experience, the transverse cervical artery can serve as an excellent arterial option with high flow and frequently allows for microvascular anastomosis without the need for vein grafting. Additionally, pedicled flaps based off the transverse cervical and supraclavicular arteries have been described for non-free flap reconstructive options. , The next distal branch of the subclavian artery is the dorsal scapular artery. Although rare, this has been used as a recipient vessel with favorable results. , Rosko and colleagues presented 3 cases in which dissection of the dorsal scapular artery in the supraclavicular triangle provided favorable vessel caliber and geometry for free flap arterial anastomosis. Importantly, authors highlight the variable anatomy with respect to the relationship between the dorsal scapular artery and the brachial plexus, underscoring the importance of careful dissection to prevent unwanted nerve injury.
Finally, the subclavian artery itself has been described as a microvascular recipient vessel using an end-to-side anastomosis. Broderick and colleagues presented a case involving recurrent carcinoma in a vessel depleted neck from prior surgery and radiation. The authors used a 2 mm punch biopsy cutter to perform an arteriotomy and proceeded with anastomosis to perfuse an anterolateral thigh free flap. It is worth nothing that such a procedure requires a long vascular pedicle owing to the relative immobility of the donor vessel. Another important consideration is the proximity of the brachial plexus and thoracic duct to the subclavian artery, increasing the risk of nervous injury and chyle leaks.
An alternative option for vessel anastomosis in the vessel depleted neck is to isolate non-cervical vessels. At our institution, as with several others, the thoracoacromial branches (deltoid, pectoralis, or other) and internal mammary artery are routinely used as a non-cervical option for arterial anastomosis. , , Although non-cervical vessels usually lie outside the radiation field, treatment plans may deliver radiation doses that extend into the upper lung fields, leading to similar difficulty utilizing the thoracic vessels. Preoperative imaging should be carefully reviewed for any evidence of radiation fibrosis within the lungs. Further, these vessel options often require long pedicled free flaps, or the use of vein grafts given the additional length traversed.
Head and neck reconstructive surgeons are often familiar with the thoracoacromial artery, especially the pectoral branch, as this provides blood supply to the pectoralis major muscle, which can be used as a pedicled flap in salvage situations with high rates of success. Use of the thoracoacromial artery as a free flap donor vessel was originally described in 2002, when Harris and colleagues described 11 free flap procedures with a 100% success rate. Martinez and colleagues later described using both the deltoid and pectoral branches of the thoracoacromial artery in microvascular reconstruction. They noted the deltoid branch had a smaller diameter than the pectoral branch; however, previous angiography studies on 10 cadavers found the pectoral and deltoid arteries to be of similar diameter (1.8 vs 1.7 mm, respectively). , Martinez and colleagues highlight that the deltoid may be preferred as it preserves the possibility of a lateral pectoralis major rotational flap. A disadvantage of using thoracoacromial branches is the limited mobility, often requiring a long flap pedicle artery. The authors, however, highlight the close proximity of the thoracoacromial system to the cephalic vein, which may be isolated concurrently.
The internal mammary arteries can be beneficial recipient vessels for head and neck reconstruction due to the high flow and volume, particularly to power vein grafts. Internal mammary vessels have consistent anatomy, allowing for ease in identification. One important consideration before utilizing the internal mammary artery is the cardiac health of the patient, as this is frequently the vessel of choice for coronary artery bypass grafting. As such, history of coronary artery bypass grafting or need for such bypass is a contraindication for use of the internal mammary artery as a flap recipient artery.
Vein grafts
Head and neck reconstruction relies on suitable recipient vessels in the neck. In scenarios when free flap pedicle length is insufficient, utilization of vein grafts is recommended. A recent multiinstitutional study examined 91 patients who required the use of an interposition vein graft and observed a success rate of 85%. Commonly, the cephalic or saphenous vein is harvested as a vein graft and can be used for both arterial and venous bridging, allowing for tension-free microvascular anastomosis. Both cephalic and saphenous veins offer a long vessel (average cephalic vein length: 18 cm; average saphenous vein length: 31 cm), consistent anatomy, and are outside of prior head and neck radiation fields. The saphenous vein, in particular, has an average diameter of 3 mm along its course, making it a suitable size match for anastomosis of many soft tissue free flaps. In cases where a smaller length of vein graft is needed, an external jugular vein can be a useful donor. , However, the diameter of the external jugular vein is often significantly larger than free flap arteries, causing anastomotic mismatch.
Long distance vein grafts can theoretically increase the rate of free flap failure due to risk of thromboses and decreased flow. Further, vein grafts require 2 sites of anastomosis, which can increase technical challenges, especially in scarred and/or irradiated tissue. At our institution, we typically utilize higher flow vessels when using vein grafts, to avoid lower flow states that can be thrombogenic. Another option is the use of a Corlett loop, a temporary arteriovenous loop created with a vein graft that provides low resistance and high flow. The midpoint of the created fistula is near the area of reconstruction to allow for recipient vessels for microvascular anastomosis. A prior study evaluated flap survival in patients with vein grafts versus Corlett loops. In their limited sample size of 36 patients, there was a 77% survival in free flaps with the vein graft technique, and 100% survival in flaps with a Corlett loop, with similar results after accounting for patients with prior radiation history. Ultimately, studies comparing these techniques are limited to small sample sizes and likely depend on many factors beyond radiation, including scar tissue, length of graft, surgeon experience, and others.
Arterial coupling
Successful anastomosis of arterial and venous circuits is the critical component of microvascular free tissue transfer and necessary for viability of the transplanted free flap tissue. Vessel anastomosis was first performed with small-diameter interrupted permanent sutures. In 1962, a mechanical coupler was described by Nakayama and colleagues; this device was further improved by Ostrup and Berggren, who reported the ability to perform both arterial and venous anastomoses in 2 to 3 minutes with a success rate of 98%. , However, early studies examining the use of this device for arterial anastomosis in head and neck free tissue transfer reported failure rates in excess of 25%. , Since these early studies, most institutions prefer to perform arterial anastomosis using small diameter suture. Our institutional preference is to use 9-0 nylon monofilament (Ethicon, Bridgewater, NJ) and we have observed a high rate of success, with overall flap failure rate of less than 2%.
In 2005, an analysis of 50 microvascular free tissue transfers for head and neck reconstruction using the Unilink Microvascular Anastomotic System (Synovis MCA, Birmingham, AL) demonstrated an overall success rate of 98% using mechanical coupler in place of free sewing for arterial anastomosis. A single intraoperative thrombosis at the site of the coupler was observed and when re-coupled, the flow was noted to be insufficient to support the transplanted tissue and the anastomosis was hand sewn. The authors demonstrated an overall reduction, although not significant, in operative time over the study duration but failed to compare their results with operative times of similar procedures in which arterial anastomosis was hand sewn. Thus, they were unable to draw conclusions about the time-saving benefits of arterial coupling. More recently, 2 groups, including our institution, have presented small case series describing the successful use of mechanical coupler in salvage scenarios. , Li and colleagues suggest the use of arterial coupling in the setting of recurrent arterial thrombosis utilizing suture and provide examples of successfully salvaged flaps using this pathway.
Estimation of free flap tissue volume
The amount of soft tissue volume to harvest for free flap reconstructive cases can be challenging to accurately predict. Relevant to head and neck defects, surgeons aim to balance the need for sufficient soft tissue coverage to allow for appropriate bulk, coverage of vital structures, and improved functional outcomes, while simultaneously maintaining adequate airway patency.
Over time, some degree of free flap tissue loss is expected due to a combination of patient age, muscle atrophy, radiation therapy, patient weight, and other factors. Intraoperatively, reconstructive surgeons empirically overestimate the free flap tissue volume needed to account for this inevitable long-term tissue loss. However, the clinical factors that account for volume loss are highly variable with each patient and thus, predicting the appropriate tissue to harvest can be challenging. A prior literature review on free tissue volume loss noted a range from 20% to 51% of non-osseous free flap tissue volume loss between 6 and 12 months posttreatment. In considering the amount of extra free flap tissue to obtain, the muscle component of a free flap undergoes more volume loss over time compared to the adipose component. Another study demonstrated that adipose volume remained at about 62.5% of tissue volume at 9 months, while muscle volume decreased to 30.2% of tissue volume at 10 months. If long-term significant tissue bulk is needed, electing for high fat-to muscle ratio on free flap design is helpful. Our institution prefers the lateral arm for this reason as well as in cosmetically sensitive reconstructions on the face due to its compartmentalized and high volume of fat that preserves well throughout treatment.
A prior study evaluated tissue volume of radial forearm and anterolateral thigh free flaps used in oral cavity and oropharyngeal defects. Volume was measured by a neuroradiologist following completion of radiation therapy, and the percentage of free flap tissue volume lost was subsequently calculated, noting a mean flap volume loss of 43%. The authors were able to create a model to predict the volume of free flap loss, achieving a small margin of error when accounting for factors such as age, sex, radiation fractionation, free flap type, and preoperative albumin level. However, being able to measure the exact volume (and muscle/adipose ratio) of tissue taken intraoperatively can be challenging to perform accurately, and often radiation dosages and/or exact fields remain unknown at this point in the patient treatment course.
Previous literature on volume tissue loss is limited based on free tissue type, patient variations, and use of radiation therapy. The effect of radiation on volume loss can be challenging to predict given the variation in radiation fractionation which may be a separate contributor to tissue loss, as well as patient post-radiation weight loss, another cause of free flap volume loss. This, compounded with the potential challenges of donor-site morbidity when additional tissue volume is taken, can make harvesting the appropriate amount of tissue challenging. Larger powered studies that account for patient and radiation factors are warranted to help guide accurate estimates of free flap volume loss of time.
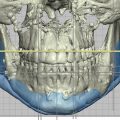
Virtual planning and modeling
Virtual planning and medical modeling is the use of computer-assisted modeling of preoperative imaging to build models and help guide resection and reconstruction. Within the realm of head and neck microvascular free tissue transfer reconstruction, virtual planning is mostly used for mandibular and midface reconstruction. It is primarily used for creating models, cutting guides to assist with tumor resection and prefabricated plates to optimize reconstructive geometry.
One of the advantages of virtual planning is improved postoperative stability. A recent small, single institution German study found that its use was associated with a significant reduction in postoperative neo-mandibular fractures when compared with conventional free hand reconstruction (0% vs 17%). Another important and well-described advantage is reduced operative time. A recent meta-analysis by Powcharoen and colleagues examined studies related to virtual planning in head and neck reconstruction. They found no significant difference in rates of postoperative complications between cases performed using conventional free hand reconstruction and those which utilized planning but did find a significant reduction in ischemia time (35 minutes), reconstructive time (2.5 minutes), total operative time (80.1 minutes), and overall length of stay (2.3 days) when it was utilized.
Critics of virtual planning note the increased cost. In 2015, Zweifel and colleagues published a study that estimated use of virtual planning increased the average cost of mandibular reconstruction by over $6000. However, when accounting for reduction in operative time associated with use of virtual planning compared to conventional reconstruction, this figured dropped to below $1500. , Additionally, more recent studies in Italy and Australia have found an overall reduction in costs when virtual planning was utilized. , These savings were explained by reduction in both operative time and length of hospitalization postoperatively. These two studies have led others to conclude that virtual planning is at least cost neutral.
Summary
Here we presented a review of the current literature related to complex head and neck free flap microvascular reconstruction. We have highlighted the abundance of nontraditional donor vessels in the challenging case of vessel depleted neck following prior cervical surgery or radiation therapy. Alternatives to traditional microvascular anastomosis including vein grafting when additional vessel length is required and use of mechanical arterial coupling in the salvage scenario, have both proved to be successful in head and neck reconstruction. Finally, we highlight important preoperative and perioperative considerations, including accurate estimation of flap volume loss and emphasized the need for additional studies and continued research in this field. Virtual planning, however, has been shown to reduce postoperative complications, operative time, and does not significantly increase the cost of the procedure.
Clinics care points
- •
When approaching a complex head and neck reconstruction, we recommend obtaining CT imaging of the neck to assist in preoperative planning with respect to vessel selection.
- •
When additional vascular lenght is needed, we reoutinley utilize the saphenous vein graft due to ease of harvest and comprable size to head and neck vasculature.
- •
We utilize commercially available virtual planning and medical modeling for the majority of cases at our institution.
- •
If utilized, surgeon must be intimately involved in the planning process to maximize the utility.
Related posts:
 Microvascular Free Flap Practice Management and Career Development
Updates in Assisted Advanced Technology for Microvascular Free Tissue Transfer in Head and Neck Surgery
Free Flap Reconstruction of the Oropharynx
Microvascular Free Flap Practice Management and Career Development
Updates in Assisted Advanced Technology for Microvascular Free Tissue Transfer in Head and Neck Surgery
Free Flap Reconstruction of the Oropharynx
 Advances in Midface Reconstruction
Advances in Midface Reconstruction
 Free Flap Enhanced Recovery Protocols in Head and Neck Surgery
Free Flap Enhanced Recovery Protocols in Head and Neck Surgery
 Custom Craniofacial Implants
Custom Craniofacial Implants
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


