Characteristics
Categories
Score
1. Amount of the infiltrated substance
Less than 200 ml
From 200 to 499 ml
From 500 ml to 1 liter
More than 1 liter
1
2
3
4
2. Infiltrated areas
One infiltrated area
From 2 to 3 infiltrated areas
More than 3 infiltrated areas
1
2
3
3. Nature of the infiltrated substance
Silicones
Biopolymers or methacrylates
Oils (edible, mineral, industrial, etc.)
Combined substances
1
2
3
4
4. Symptoms
Local inflammation (pain, heat, erythema)
Fever and generally unwell (asthenia, adynamia and weight loss)
Autoimmune disease
Pneumopathy
1
1
1
1
5. Signs
Presence of nodules
Substance migration
Hyperpigmentation and stiffening of the skin
Ulceration or infection
1
1
1
1
6. Laboratory studies
Normal studies
Leukopenia
High C-reactive protein level
Increase in erythrocyte-sedimentation rate
Multiple organ failure (hepatic, renal, blood)
0
1
1
1
1
7. Magnetic resonance imaging
Skin and the subcutaneous tissue involvement
Muscle involvement
Involvement of other organs
1
1
1
Clinical stages of disease caused by the injection of silicone or other oils, categorized by the summation score for the seven characteristics listed in Table 7.1
Clinical stages | Characteristics | Surgery | Prognosis |
|---|---|---|---|
Stage 1 (from 6 to 10) | Excellent response to immunomodulatory-pharmacological treatment (methotrexate, meticorten, colchicine, folic acid) | No | Good |
Stage 2 (from 11 to 17) | Good response to pharmacological treatment. After 6 months, the infiltrated tissues improved (less hard, less pigmented, better circulation, etc.) | Yes, try to remove siliconomas | Reserved. Successful reconstruction possible |
Stage 3 (from 18 to 23) | Limited response to pharmacological treatment. Poor circulation, fibrous tissues and little elasticity. Poor healing | Yes, try to remove siliconomas | Limited. High rate of complications |
Stage 4 (from 24 to 26) | Urgent hospitalization. No significant response to drug treatment. Not candidates for any surgical treatment | No | Poor short term. Very serious. May die from multiple organ failure |
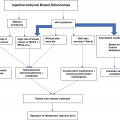
The decision regarding what form or forms of treatment to offer must be adapted to each patient’s clinical stage, since the presenting clinical manifestations of disease produced by the injection of oils or silicones are usually insidious, with nonspecific clinical and serological alterations, an unpredictable clinical course, and alternating symptomatic and asymptomatic periods (Table 7.2).
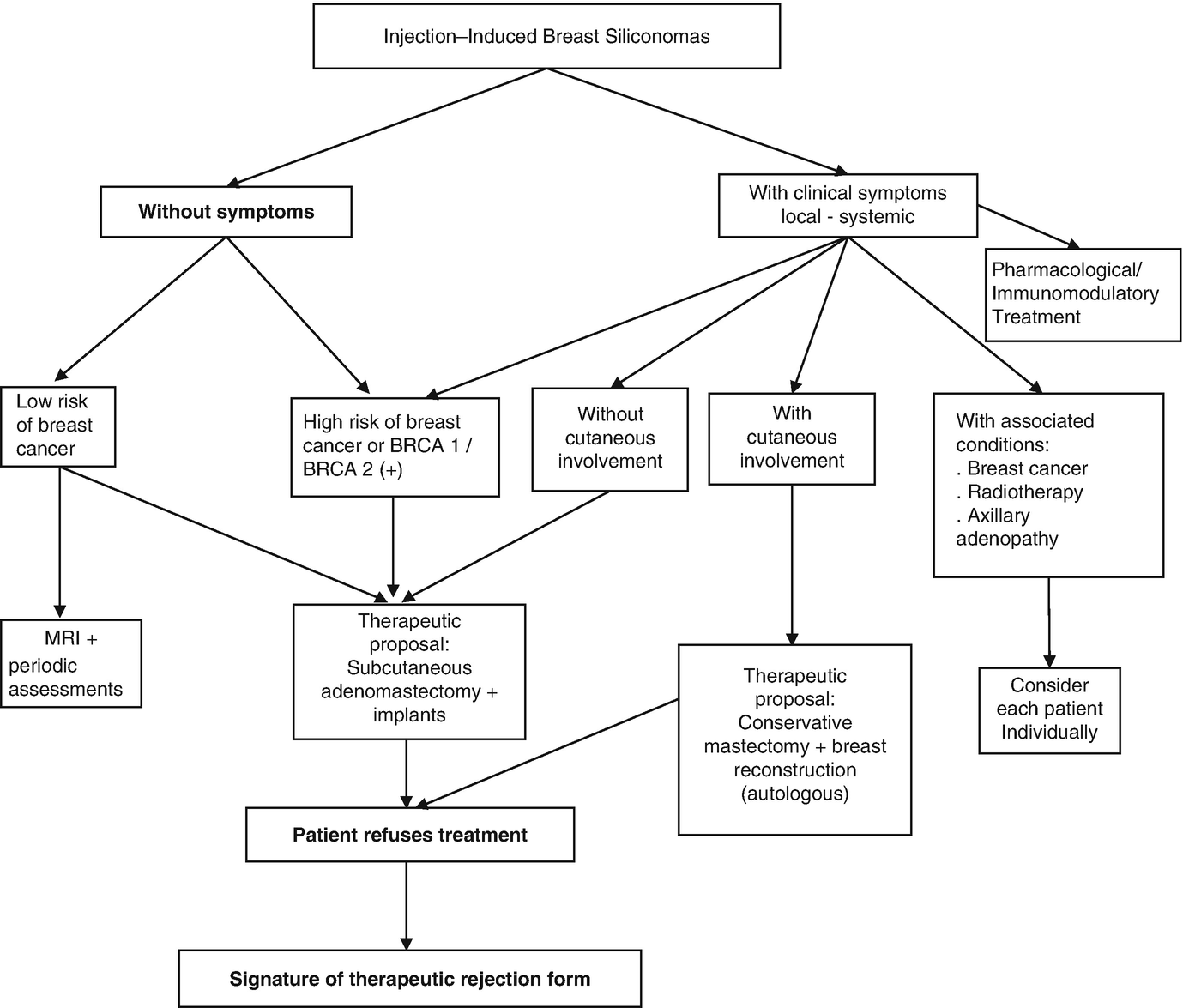
For the treatment of silicone-induced axillary lymphadenopathy, we have designed another axillary-specific therapeutic algorithm that will be discussed at length in Chap. 14.
We followed the same guidelines provided in Chap. 5, where we described the diverse presentations of disease caused by liquid silicone injections, organized using a logical sequence of tissue and systemic compromise: from the mildest forms through to the most serious forms of damage, where the patient’s disease seriously impacts their quality of life and poses risks to life itself.
We will now present the appropriate therapeutic approaches for each form of mammary siliconoma presentation. Rather than forcing readers to refer back to photographs used in Chap. 5, some of those same photographs will be used here.
Patients with No Mammary Cutaneous Involvement (Figs. 7.1, 7.2, 7.3, 7.4, 7.5, and 7.6)

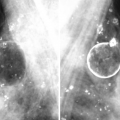
Mammary siliconomas after the injection of liquid silicone throughout the mammary gland. An asymptomatic patient

Breast siliconomas after the injection of liquid silicone. An asymptomatic patient, with collapsible skin not infiltrated by silicones. Note the multiple painful palpable nodules distributed throughout the breast parenchyma
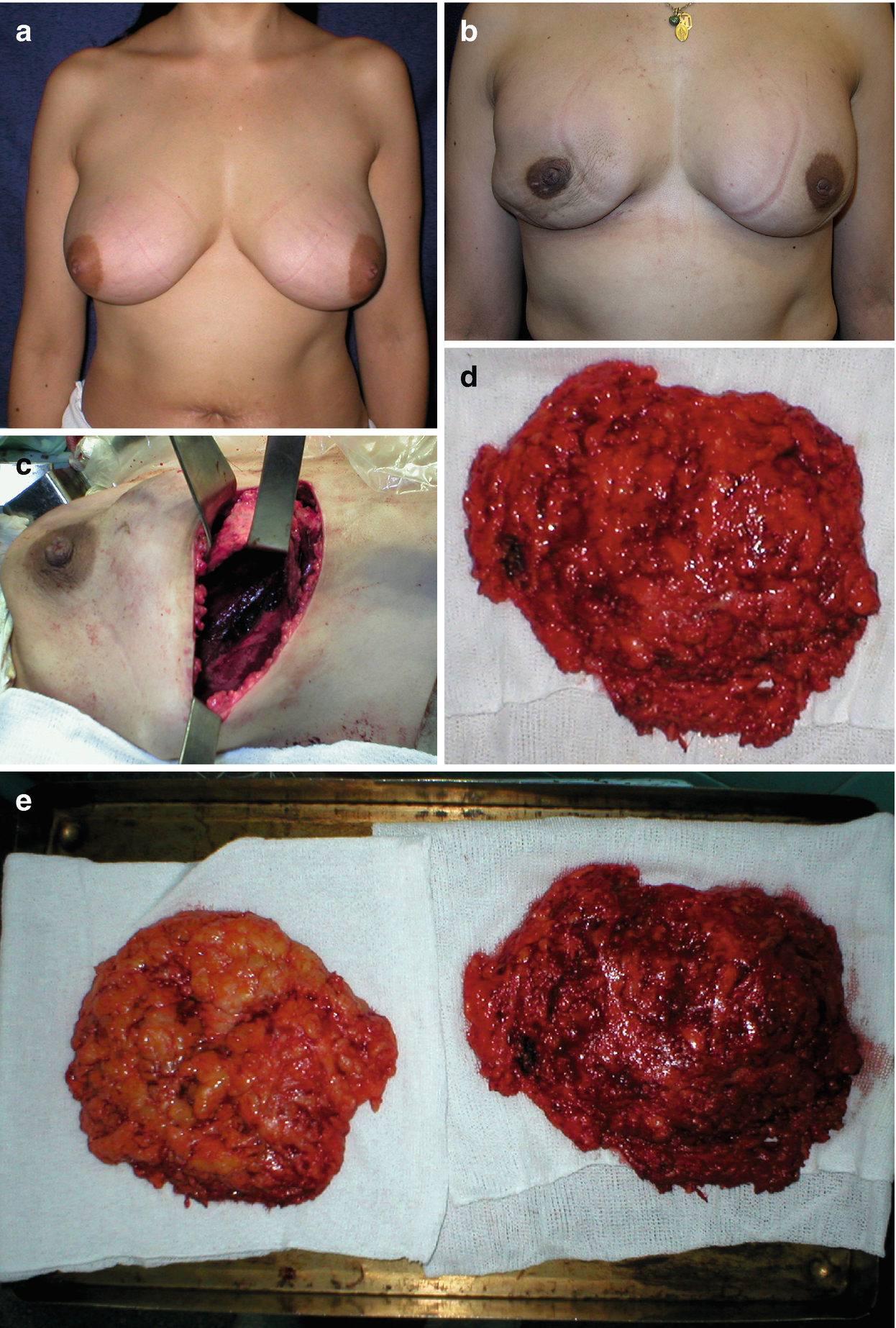
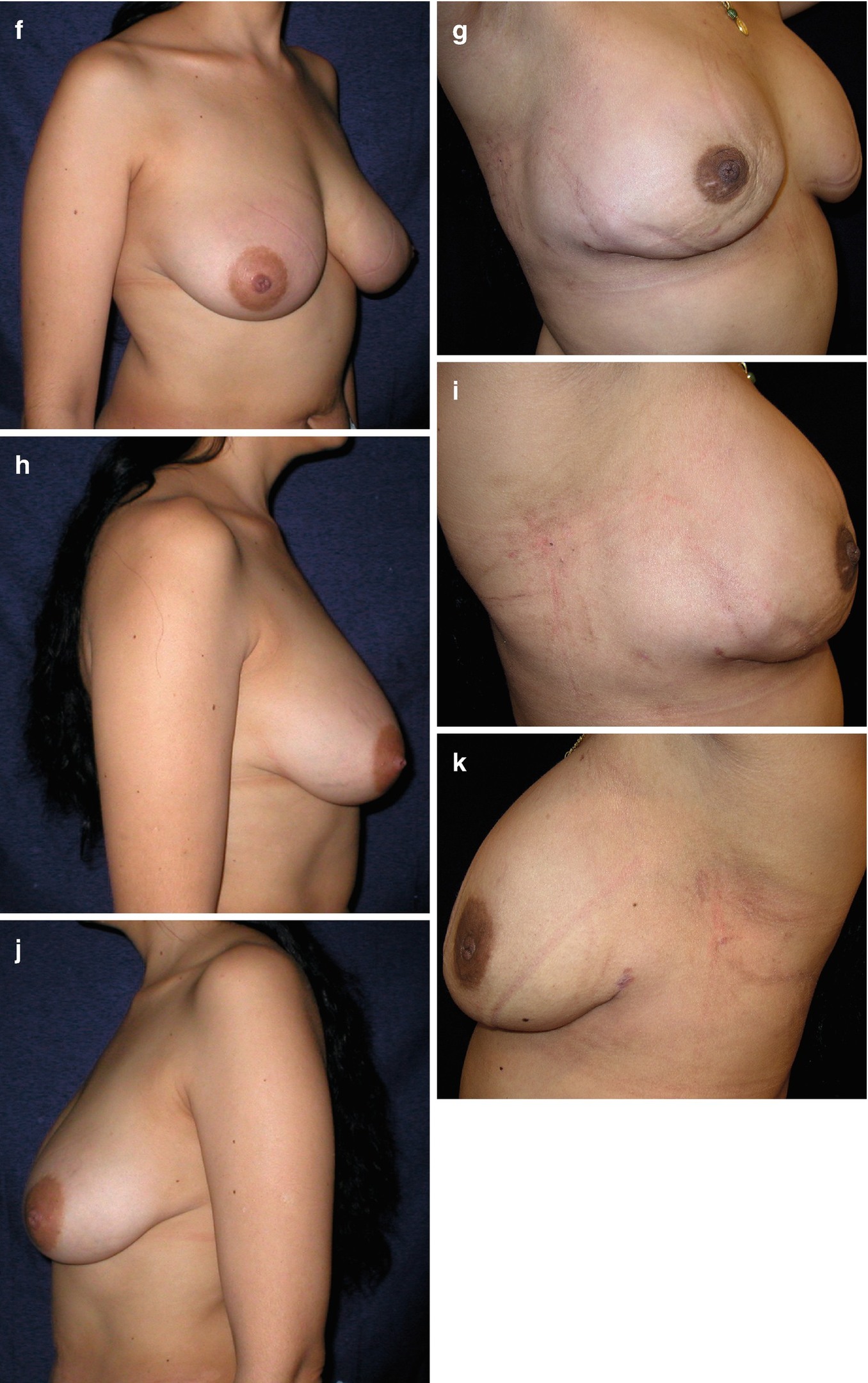
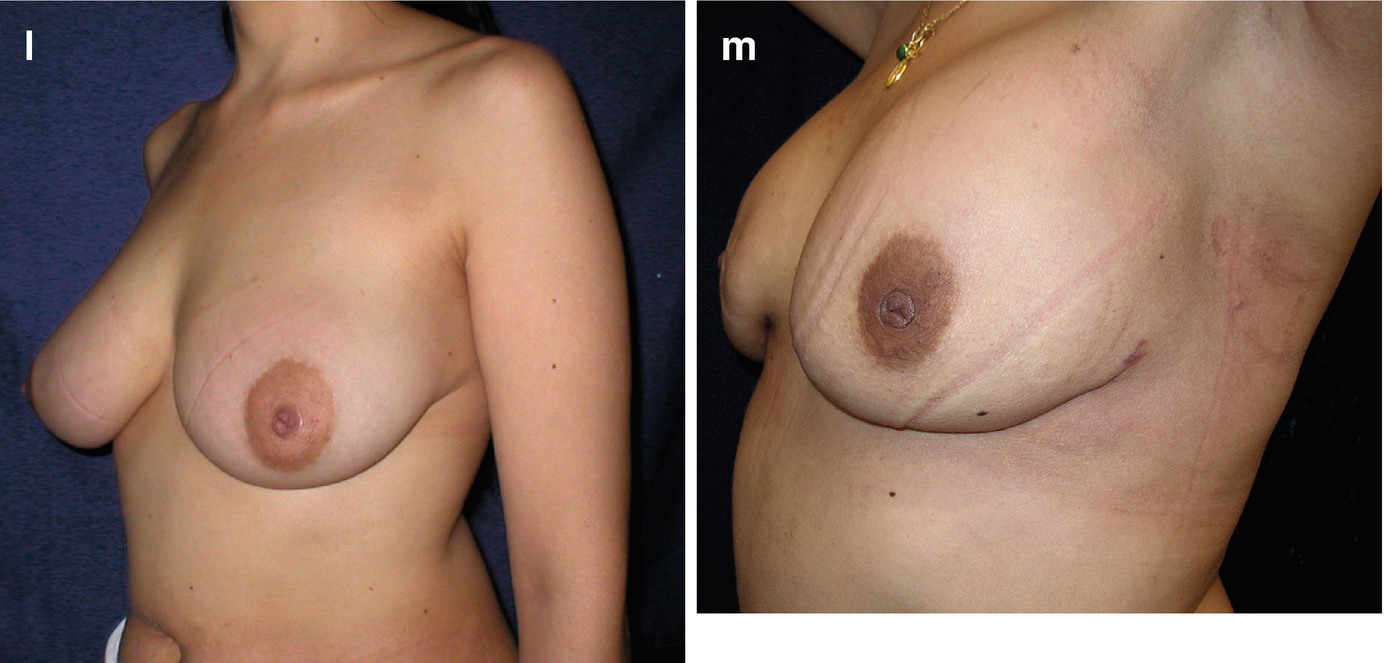
Breast siliconomas after the injection of liquid silicone. An asymptomatic patient. Note the mammary erythema. (a) Preoperative, front view. (b) Postoperatively after a subcutaneous adenomastectomy, with a wide submammary incision. The postoperative appearance was deemed satisfactory, but inferior to the appearance preoperatively. (c) Intraoperative view of the subcutaneous adenomastectomy. Close-up of the total retromuscular pocket. (d, e) Surgical specimens. (f) Preoperative view, three-quarter profile. (g) Postoperative view,three-quarter profile. (h) Preoperative side view. (i) Postoperative side view. (j) Preoperative side view. (k) Postoperative side view. (l) Preoperative view, three-quarter profile. (m) Postoperative view, three-quarter profile
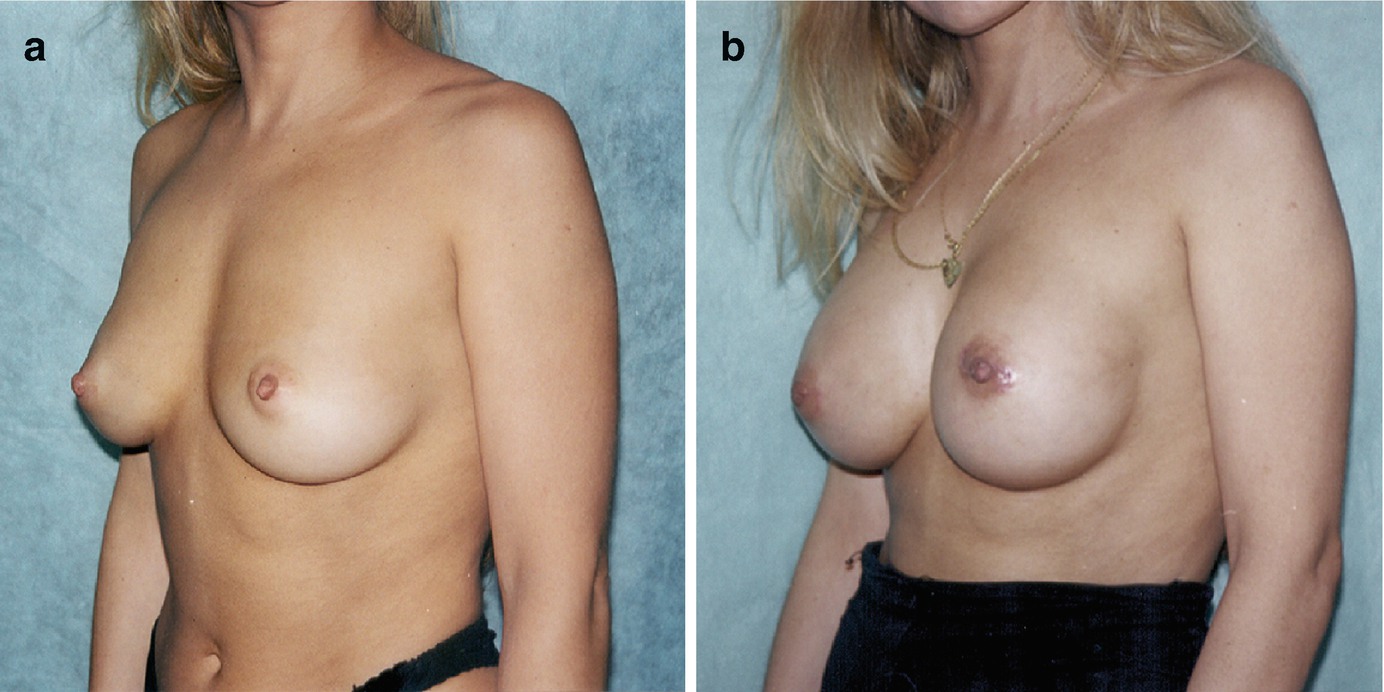
(a) Breast siliconomas: preoperatively. (b) Postoperatively after an adenomastectomy via an inferior periareolar incision, with subsequent reconstruction using silicone gel implants. The postoperative appearance was aesthetically inferior to that preoperatively
Patients Who Reject Reconstruction with Implants
Many patients reject reconstruction with breast prostheses for fear of replacing silicone with silicone or for economic reasons.
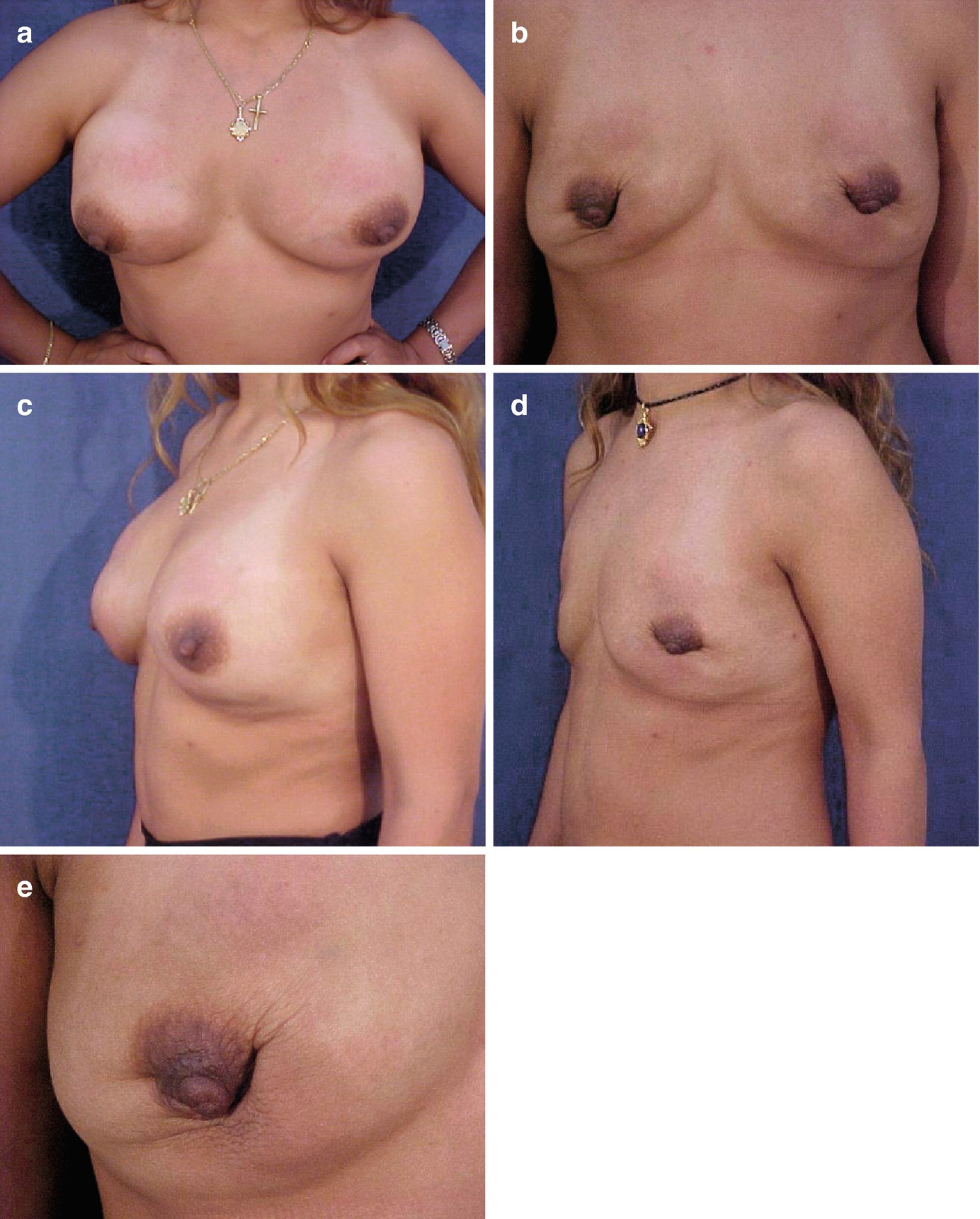
Mammary siliconomas with mild cutaneous involvement. Erythema and multiple painful breast masses. (a) Preoperative front view. (b) Postoperatively, post bilateral adenomastectomy through the inferior periareolar pathway, without reconstruction: aesthetic sequela of adenomastectomy without implants (front view). (c) Preoperative view, three-quarter profile. (d) Postoperative view, three-quarter profile. (e) Close-up of the aesthetic sequelae

(a) Mammary siliconomas without cutaneous involvement; flexible skin. Surgical plan: adenomastectomy with skin preservation through the inferior periareolar route; given the generous breast volume and good abdominal musculature, immediate reconstruction was performed with a bilateral desepidermized TRAM flap. (b) Postoperative complication: central necrosis of the abdominal flap with exposure of the proline mesh that reconstructs the muscle defect; healing by second intention. (c) Preoperative side view. (d) Postoperatively: note the scar secondary to central necrosis of the abdominal flap
Patients with Mammary Cutaneous Involvement
Involvement Limited to the Lower Breast Quadrant (Figs. 7.7 and 7.8)
Wise Pattern Involvement (move to the top of the next paragraph)
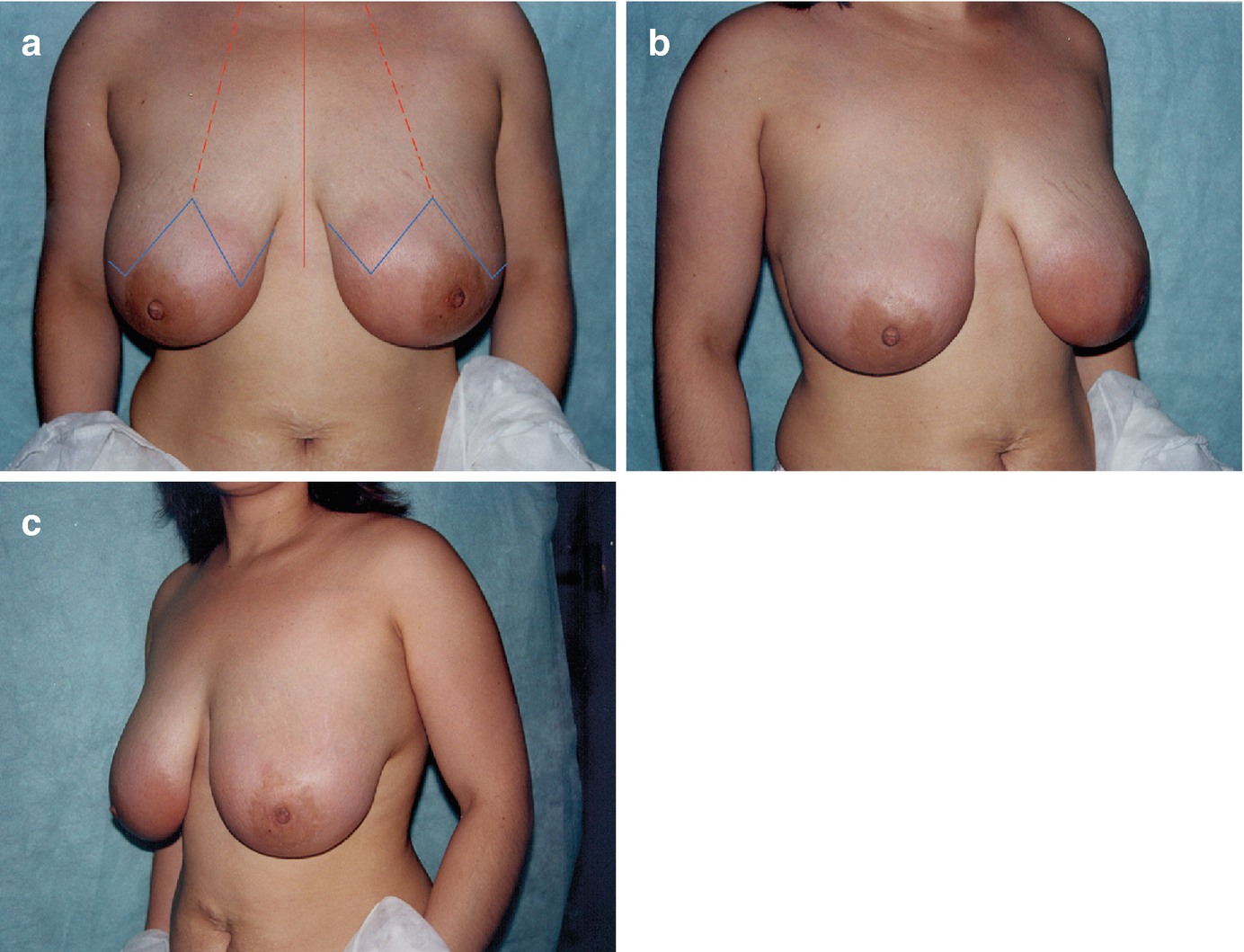
Mammary siliconomas with extensive skin involvement: orange peel skin secondary to lymphoedema. (a) Front view. Planned resection with a Wise pattern, accommodating the extent of skin involvement due to silicone infiltration. (b, c) Side views
Cutaneous Involvement that Exceeds Wise’s Pattern but Remains Limited to the Breast
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


