The safety, efficacy, and rapid recovery of conscious sedation/local anesthesia make this anesthetic technique useful in the ambulatory setting. The care of the sedated patient requires a team effort. The individual role and responsibility of patient, surgeon, anesthesia provider, and nursing staff are discussed. Using data obtained from a series of 1400 consecutive cases, the authors’ experience with conscious sedation/local anesthesia is presented. The current technique, using low-dose propofol, is described in detail. Using conscious sedation, the patient’s level of consciousness is depressed, but respiratory drive and airway reflexes are maintained and anesthesia is provided by infiltration of local anesthetic.
Key points
- •
Conscious sedation/local anesthesia is a challenging technique requiring cooperation of the patient, surgeon, and anesthesia provider.
- •
The anesthesia provider keeps the patient sedated, whereas the surgeon provides the anesthesia (local).
- •
In the authors’ experience, the defining factor of “conscious sedation” is the ability of the patient to maintain spontaneous respirations and the ability (reflexes) to protect the airway throughout the procedure.
- •
The properties of propofol, especially the rapid onset and short duration of action, make it an ideal agent for conscious sedation.
- •
Because the level of sedation can deepen unexpectedly with propofol, an anesthesia provider should administer and monitor the patient.
- •
Low-dose propofol conscious sedation with local anesthesia is a safe and effective anesthetic for a wide spectrum of surgical procedures.
- •
It is the dose of the drug, not the route of administration, which determines depth of sedation.
- •
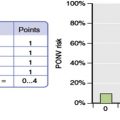
PONV is infrequent with this technique.
With the increasing number of office-based surgical (OBS), medical, and diagnostic procedures done each year, there has been resurgence in the use of intravenous sedation. The American Association for the Accreditation of Ambulatory Surgical Facilities (AAAASF), which provides accreditation for most OBS and office-based medical facilities in the United States, has demonstrated the safety of OBS from peer review data involving more than 1 million procedures. Several independent reports have confirmed the safety of ambulatory surgery.
Current anesthetic methods, improved monitoring technology, and newer drugs have improved the safety of general anesthesia and that of intravenous sedation. The importance of OBS facility accreditation and appropriate physician credentialing for patient safety cannot be overemphasized and are integral to the conclusions of this article. In fact, when propofol is used, AAAASF requires a credentialed anesthesia provider to administer the anesthetic and that the facility be equipped comparably with one approved for general anesthesia.
Intravenous sedation encompasses a broad continuum of levels of consciousness, from a low-dose tranquilizer reducing anxiety in an awake patient, to deep sedation requiring supplemental oxygen and airway management. Measurable outcomes of conscious sedation (midazolam/fentanyl) and deep (propofol) sedation have been found to be effective and safe in a series reported by Hansen and coworkers. This article presents the authors’ extensive experience with conscious sedation/local anesthesia as a safe, comfortable, and effective but constantly evolving technique. Because conscious sedation requires teamwork, the discussion includes the perspective of the various members of the operating room (OR) team.
Conscious sedation defined
According to the American Society of Anesthesia, “Conscious sedation is a drug-induced depression of consciousness during which patients respond purposefully to verbal commands, either alone or accompanied by light tactile stimulation. No interventions are required to maintain a patent airway, and spontaneous ventilation is adequate. Cardiovascular function is usually maintained.” This is in contrast to deep sedation, in which the patient is unconscious and requires assistance with airway management, with potential impairment of cardiovascular function. Many surgeons prefer deep sedation because it requires less time and concern for patient comfort than conscious sedation. However, deep sedation increases the risk of airway compromise, incidence of postoperative nausea and vomiting (PONV), and recovery time. It could be argued that deep sedation is merely a “light general anesthetic” and should be treated as such with mechanical control of the airway. Conscious sedation, properly administered, is safer, has a lower incidence of PONV, and provides a shorter recovery.
In the authors’ experience, the defining factor of conscious sedation is the ability of the patient to maintain spontaneous respirations and the ability (reflex) to protect the airway. Although the authors’ patients are generally responsive to verbal and physical stimuli most of the time, they are maintained at a deeper level during the initial injection of the local anesthesia and occasionally and briefly at intervals of more intense stimulation. Occasionally, it is necessary to lift the jaw to temporarily maintain the airway, but the need to use a mask for positive pressure assistance was uncommon in the authors’ series. In their experience, supplemental oxygen, which is potentially dangerous because of fire hazard, is not required, because no patient has exhibited hypoxia requiring the use of intubation. Intraoral and intranasal airways are not routinely used. Of interest, Stemp has suggested that supplemental oxygen can actually be detrimental because it can mask and delay the diagnosis of hypoventilation.
Conscious sedation/local anesthesia is a challenging technique requiring cooperation between the surgeon and anesthesia provider. The nonthreatening office environment, with limited anesthesia equipment, recovery space, and personnel requirements, together with the reduced incidence of PONV and shorter recovery time, make this technique ideal for OSB procedures. Significantly, certain risks of general anesthesia can be reduced or avoided with the use of conscious sedation, including deep vein thrombosis, pulmonary complications, OR fires, and pressure injuries. The cost effectiveness of OBS and conscious sedation is crucial as hospital costs increase, despite shrinking health care resources. In cosmetic surgery, the use of conscious sedation and OBS can provide a valuable marketing advantage to the surgeon, including safety, cost, and patient satisfaction. Empirically, the risk of deep venous thrombosis in a sedated patient should be negligible compared with general anesthesia. However, it is the authors’ practice and an AAAASF requirement to use a sequential compression device on all cases lasting longer than an hour.
In some practices, oral sedation is used for OBS to avoid the necessity of accreditation, which is mandated in many states for facilities using intravenous sedation. However, most oral drugs have relatively long onset and duration, making the control of level of consciousness unpredictable. Furthermore, the occurrence of an overdose is difficult to manage without trained personnel and the availability of adequate resuscitation drugs and equipment. AAAASF requires the continual monitoring of vital signs, oxygenation, and continuous monitoring of electrocardiogram by a qualified physician when using sedation. It is important to understand that the depth of sedation is related to dose, not route of administration of the sedating drug.
Conscious sedation defined
According to the American Society of Anesthesia, “Conscious sedation is a drug-induced depression of consciousness during which patients respond purposefully to verbal commands, either alone or accompanied by light tactile stimulation. No interventions are required to maintain a patent airway, and spontaneous ventilation is adequate. Cardiovascular function is usually maintained.” This is in contrast to deep sedation, in which the patient is unconscious and requires assistance with airway management, with potential impairment of cardiovascular function. Many surgeons prefer deep sedation because it requires less time and concern for patient comfort than conscious sedation. However, deep sedation increases the risk of airway compromise, incidence of postoperative nausea and vomiting (PONV), and recovery time. It could be argued that deep sedation is merely a “light general anesthetic” and should be treated as such with mechanical control of the airway. Conscious sedation, properly administered, is safer, has a lower incidence of PONV, and provides a shorter recovery.
In the authors’ experience, the defining factor of conscious sedation is the ability of the patient to maintain spontaneous respirations and the ability (reflex) to protect the airway. Although the authors’ patients are generally responsive to verbal and physical stimuli most of the time, they are maintained at a deeper level during the initial injection of the local anesthesia and occasionally and briefly at intervals of more intense stimulation. Occasionally, it is necessary to lift the jaw to temporarily maintain the airway, but the need to use a mask for positive pressure assistance was uncommon in the authors’ series. In their experience, supplemental oxygen, which is potentially dangerous because of fire hazard, is not required, because no patient has exhibited hypoxia requiring the use of intubation. Intraoral and intranasal airways are not routinely used. Of interest, Stemp has suggested that supplemental oxygen can actually be detrimental because it can mask and delay the diagnosis of hypoventilation.
Conscious sedation/local anesthesia is a challenging technique requiring cooperation between the surgeon and anesthesia provider. The nonthreatening office environment, with limited anesthesia equipment, recovery space, and personnel requirements, together with the reduced incidence of PONV and shorter recovery time, make this technique ideal for OSB procedures. Significantly, certain risks of general anesthesia can be reduced or avoided with the use of conscious sedation, including deep vein thrombosis, pulmonary complications, OR fires, and pressure injuries. The cost effectiveness of OBS and conscious sedation is crucial as hospital costs increase, despite shrinking health care resources. In cosmetic surgery, the use of conscious sedation and OBS can provide a valuable marketing advantage to the surgeon, including safety, cost, and patient satisfaction. Empirically, the risk of deep venous thrombosis in a sedated patient should be negligible compared with general anesthesia. However, it is the authors’ practice and an AAAASF requirement to use a sequential compression device on all cases lasting longer than an hour.
In some practices, oral sedation is used for OBS to avoid the necessity of accreditation, which is mandated in many states for facilities using intravenous sedation. However, most oral drugs have relatively long onset and duration, making the control of level of consciousness unpredictable. Furthermore, the occurrence of an overdose is difficult to manage without trained personnel and the availability of adequate resuscitation drugs and equipment. AAAASF requires the continual monitoring of vital signs, oxygenation, and continuous monitoring of electrocardiogram by a qualified physician when using sedation. It is important to understand that the depth of sedation is related to dose, not route of administration of the sedating drug.
Clinical experience
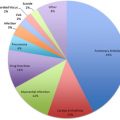
Fifteen years experience of 1400 consecutive cases done by a nurse anesthetist in a single practice Class B AAAASF OBS facility were retrospectively reviewed for incidence of anesthetic complications, fatalities, and unanticipated hospital admissions. Drugs used, doses given, and order of administration varied; however, the technique described here has evolved over the past 15 years and has proved effective and safe. Table 1 shows the low incidence of complications of conscious sedation with local anesthesia. Several series have been published that mirror these data and conclusions. Our data show that the routine use of supplemental oxygen for patients under conscious sedation is unnecessary. However, if the anesthesia provider prefers the use of supplemental oxygen, recent studies suggest a nasopharyngeal catheter may be safer than other delivery methods.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


