The most common plastic surgery-related congenital conditions of the lower extremity are: constriction ring, lymphedema, syndactyly, nevi, and vascular anomalies. Principles of reconstruction are based on the condition and type of deformity. The pediatric population typically has less co-morbidities than adults that can negatively affect outcomes (eg, diabetes, peripheral vascular disease), although children can be less compliant with postoperative care. Growth, development, appearance, and postoperative compliance are variables that especially influence operative management of children.
Key points
- •
The most common congenital leg conditions managed by plastic surgeons are constriction ring, syndactyly, lymphedema, nevi, and vascular anomalies.
- •
Principles of management generally follow adult lower limb reconstruction with special considerations for long-term functional and aesthetic outcomes.
- •
Immobilization of the extremity can help ensure protection of the limb postoperatively.
Introduction
The most common congenital anomalies of the legs managed by plastic surgeons are: syndactyly, constriction rings, lymphedema, congenital nevi, and vascular anomalies. Because of the pediatric age group, aesthetic outcomes are particularly emphasized by patients and families. Diagnosis of congenital lower extremity disorders is made by history and physical examination; imaging and histopathology are rarely needed. Indications for operative management are based on the type of congenital condition.
Congenital anomalies do not require operative intervention unless they are causing a functional or “cosmetic” problem. The lower extremity is an unfavorable location to remove large lesions of the integument because skin redundancy is minimal and gravity favors swelling, which increases stress on the incision line. It is best to perform elective procedures after 6 mo of age because the infant’s physiology approximates that of an adult, which reduces the risk of anesthesia. Because most infants begin ambulating around 12 mo of age, it is preferable to remove lesions before this time to reduce the risk of suture line dehiscence. If patients present after 12 mo of age with lesions causing a deformity only (eg, infantile hemangioma, benign pigmented nevus), then removing the lesion before 4 y of age will eliminate the deformity before the child’s long-term memory and self-esteem begins to form. Some parents will prefer to wait until a child is old enough to participate in the decision to extirpate a lesion, which can occur in late childhood or early adolescence.
Advantages of performing lower extremity reconstruction in children are that they typically do not have adult co-morbidities that can complicate operations (eg, smoking history, diabetes, and peripheral vascular disease). Because the pediatric population does not have arterial or venous disease, they can best tolerate wide skin undermining and closure of wounds linearly. A disadvantage of surgery in the pediatric population is that patients are less likely to follow postoperative instructions. Consequently, immobilization of the extremity should be performed after an operation. Children and their parents are less tolerant of scars and the aesthetic outcome is more of a focus compared to adults. For example, patients often return requesting scar revisions and excision of skin grafts because they are concerned with their appearance, particularly during adolescence. Children’s legs are often exposed during school or sports and their peers can comment on their deformity. Consequently, the pediatric population can require more revisions to achieve the best aesthetic result compared to adult patients.
Constriction ring
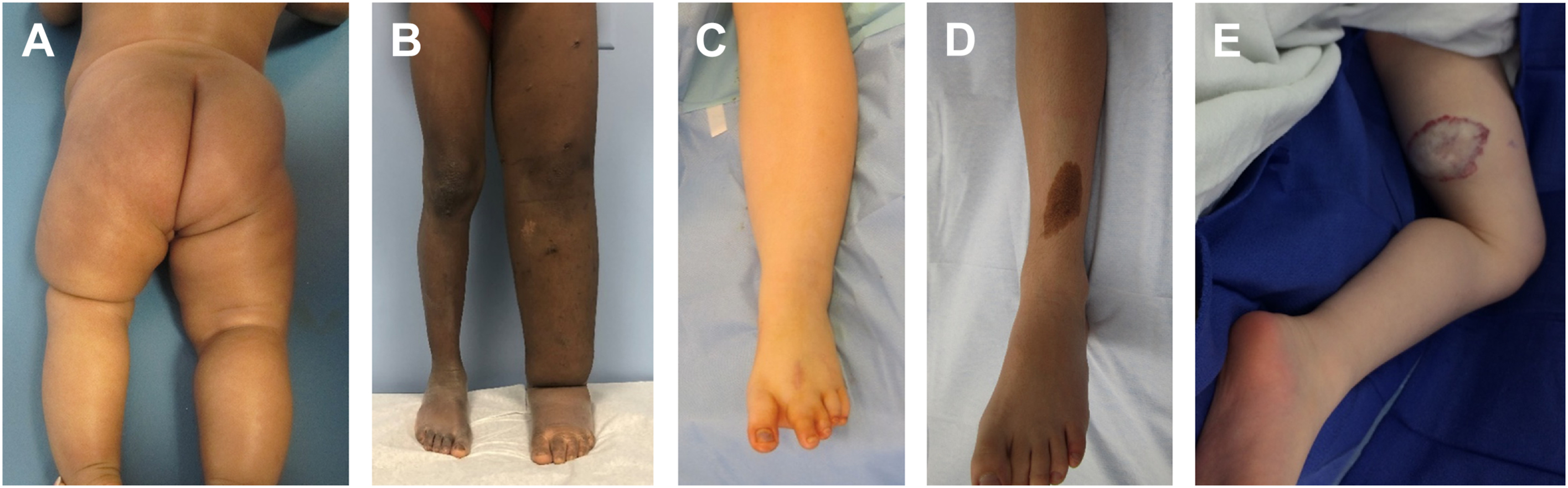
Constriction ring is most common in the toes but can affect any area of the leg ( Fig. 1 ). The spectrum ranges from superficial scarring to deep bands. Functional disability, growth disturbance, joint deformity, lymphedema, and congenital amputation can occur. Operative management is indicated to improve the appearance of a deformity, as well as to correct any functional problems. Mild constriction rings do not require intervention.
Operative treatment of a constriction ring should address the functional and aesthetic issues of the limb. Collaboration with an orthopedic surgeon is required in cases of joint involvement. For bands involving the legs or thighs, excision and flap advancement is performed. It is most favorable to treat prior to ambulation to take advantage of the extra soft tissue of an infant and easier immobilization.
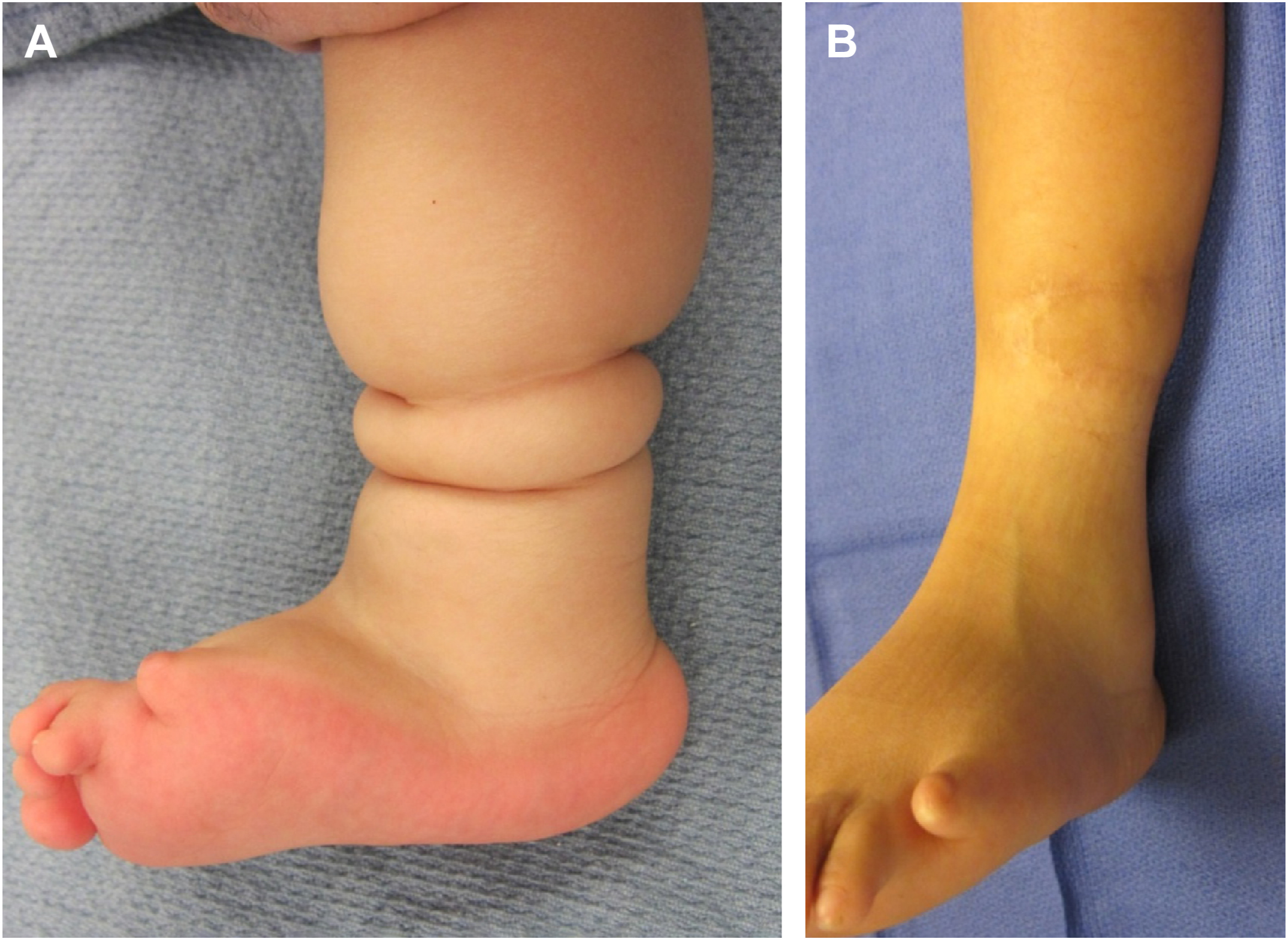
Bands that are deep and narrow are favorable because they provide extra soft tissue to restore contour. The ring is marked and the skin is excised. Separate adipofascial and skin flaps are raised. The adipofascial flaps are mobilized and closed and then the skin flaps are approximated ideally away from the line of closure of the adipofascial flaps. Z-plasties are advocated extensively in the literature but are rarely needed. If the ring is deep or if there are multiple closely-spaced rings, then a staged approach is performed ( Fig. 2 ).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


