What structures develop from the hillocks of the first branchial arch?
The tragus, the helical crus, and helical root (lymphatic drainage to parotid nodes).
 What structures develop from the three hillocks of the second branchial arch?
What structures develop from the three hillocks of the second branchial arch?
The helix, scapha, concha, antihelix, antitragus, and lobule (lymphatic drainage to posterior auricular nodes). The most common auricular sinus lies at the junction between the helical root and the superior helix (rises at the boundary between the first and second arch contributions).
 What embryologic structure gives rise to the external auditory meatus?
What embryologic structure gives rise to the external auditory meatus?
The first branchial groove (lymphatic drainage to both parotid and posterior auricular nodes).
 What is the normal size of the ear?
What is the normal size of the ear?
5.5 to 6.5 cm for the normal adult ear height and 3 to 4.5 cm for the normal adult ear width. The width varies from 66% of the height in children to 55% of the height in adults. For children 4 years of age, a subnormal ear height (i.e., <2 SD) is below 4.5 cm.
 Describe normal ear growth.
Describe normal ear growth.
85% of ear development occurs by 3 years of age with full development achieved between 6 and 15 years of age.
 What is the normal position of the ear?
What is the normal position of the ear?
1. One ear length posterior to the lateral orbital rim.
2. Mean inclination from vertical of 20-degree posteriorly.
 What is the normal scalp-to-helix distance for each third of the ear? (Upper, middle, and lobule)
What is the normal scalp-to-helix distance for each third of the ear? (Upper, middle, and lobule)
1. Upper: 1.0 to 1.2 cm
2. Middle: 1.6 to 1.8 cm
3. Lobule: 2.0 to 2.2 cm
 How is the concha subdivided?
How is the concha subdivided?The concha cavum and concha cymba, which are separated by the helical root (also referred to as the root of the helical crus).
 The superior crus of the antihelix is bordered by what structures?
The superior crus of the antihelix is bordered by what structures?
The scapha and the triangular fossa.
 The inferior crus of the antihelix is bordered by what structures?
The inferior crus of the antihelix is bordered by what structures?
The triangular fossa and the concha cymba.
 What is the triangular fossa?
What is the triangular fossa?
The concave area between the superior crus and the inferior crus.
 Describe the arterial blood supply to the ear.
Describe the arterial blood supply to the ear.
Superficial temporal artery supplies the anterior surface. Posterior auricular artery supplies the posterior surface of the ear, lobule, and retroauricular skin. There are numerous perforating vessels interconnecting the two territories.
 Describe the venous drainage of the ear.
Describe the venous drainage of the ear.
Anterior ear is drained by the superficial temporal and retromandibular veins. Posterior ear is drained by posterior auricular veins draining into the external jugular vein.
 Describe the innervation of the ear (Fig. 66-1).
Describe the innervation of the ear (Fig. 66-1).
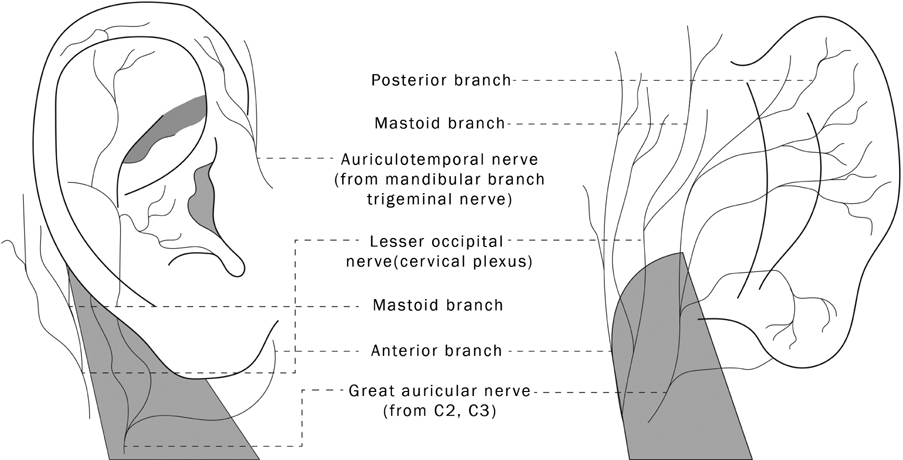
Figure 66-1 Innervation of the ear.
*Illustrations by Matthew Gould.
Sensory supply of the anterior surface of the ear is via the auriculotemporal (V3) and great auricular (CN II–III) nerves. The posterior surface is innervated by the great auricular nerve, and the mastoid branches of the lesser occipital nerve. The region of the meatus (and medial concha) is supplied by the nerve of Arnold from the Vagus nerve (oropharyngeal cancer may present with referred pain to the ear via vagal nerve fibers common to the oropharynx and concha).
 Microtia is seen in what syndromes (Fig. 66-2)?
Microtia is seen in what syndromes (Fig. 66-2)?
Figure 66-2 Microtia.
1. Hemifacial microsomia (first and second branchial arch syndrome).
2. Goldenhar syndrome (oculoauriculovertebral dysplasia; characteristically has bilateral ear deformities).
3. Treacher Collins syndrome (bilateral deformities).
 What is the proposed pathogenesis of microtia?
What is the proposed pathogenesis of microtia?
Obliteration of the stapedial artery. The bilateral deformity in Treacher Collins syndrome has been demonstrated to arise from a different event occurring early in gastrulation (Poswillo) and has also been associated with thalidomide.
 For the microtia patient, at what age is it usually recommended for the child to undergo total ear reconstruction?
For the microtia patient, at what age is it usually recommended for the child to undergo total ear reconstruction?
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


