Structural preservation rhinoplasty (SPR) uses structural methods and dorsal preservation. SPR approaches include (1) dorsal preservation techniques coupled with structural approaches to the lower third/nasal tip complex; (2) use of structural methods to convert a nasal dorsum to a preservation candidate; (3) preservation ideology applied to structural tip pasty, emphasizing suture modification and limited resection; (4) minimization of the degree of soft tissue disruption at the middle vault and dorsum in preservation and structural cases; (5) modified dorsal preservation techniques in which some components of the nasal dorsum are treated with structural methodology while others are treated with preservation methods.
Key points
- •
Structural preservation rhinoplasty (SPR) incorporates the benefits of preservation and structural rhinoplasty and has several variations.
- •
Dorsal preservation can be effectively coupled with structural lower-third and nasal tip modifications.
- •
A preservation lens should be used when applying structural methods.
- •
A nasal dorsal convexity can be converted to a preservation candidate using structural techniques (eg, osteoplasty or grafting).
- •
Modified dorsal preservation techniques use partial preservation of either the midvault or nasal bone-upper lateral cartilage junction and incorporate structural methods.
| DOHM | dorsal osseocartilaginous horizontal mattress |
| DPR | dorsal preservation rhinoplasty |
| DSG | dorsal septal gap |
| LD | let-down |
| MSSM | modified subdorsal strip method |
| PD | push-down |
| PR | preservation rhinoplasty |
| SMAS | sub-superficial musculoaponeurotic system |
| SPR | structural preservation rhinoplasty |
| SR | structure rhinoplasty |
| ULC | upper lateral cartilage |
Introduction
Preservation rhinoplasty (PR), in contrast to structure rhinoplasty (SR), aims to preserve rather than violate key endogenous attributes of the nose including cartilage, soft tissue, and ligaments. Dorsal preservation (DPR) specifically refers to the en bloc lowering of the dorsum with conservation of the nasal keystone, with or without modification of the bony cap. Several studies have shown good patient satisfaction with dorsal preservation methods, as well as low rates of revision surgery, residual or recurrent hump, postoperative nasal deviation, and postoperative infection. In light of this, there has been a resurgence in the implementation of preservation techniques in rhinoplasty. However, there are scenarios in which structural rhinoplasty may be better indicated for treatment of the dorsum and/or nasal tip.
In some DPR cases, modulation of certain aspects of the nose with structural techniques may better achieve desirable contours and outcomes. This philosophy has become known as structural preservation rhinoplasty (SPR), in which structural methods and dorsal preservation are used in the same patient. , In previous descriptions of this approach, the nasal dorsum and midvault are managed via preservation techniques, while the lower third of the nose/nasal tip is treated with primarily structural techniques. The fusion of techniques allows for greater versatility and gives surgeons familiar with structural techniques the ability to incorporate certain preservation principles, primarily DPR, into practice. This article reviews the philosophy, indications, and techniques associated with SPR.
General concepts in structural preservation rhinoplasty
Although structural rhinoplasty is the more ubiquitous rhinoplasty approach at this time, the use of preservation techniques is becoming more pervasive. Despite its equally long history, few rhinoplasty surgeons actively incorporate dorsal preservation into their practices. In recent years, with an increase in education and exposure surrounding preservation, there has been a growing appreciation for this methodology and its associated benefits. The fusion of preservation and structural rhinoplasty reflects an important technical advancement in nasal surgery, as it acknowledges the benefits of each approach and allows for increased versatility.
Fundamentally, preservation surgery endorses 3 major concepts. As aforementioned, DPR minimizes violation of the keystone and the attachments of the upper lateral cartilages (ULCs) to surrounding structures. As such, the bony and cartilaginous vaults are treated as 1 unit, and there is no need for midvault reconstruction. Secondly, sub-perichondrial dissection is favored; soft tissue and nasal ligaments are preserved where possible and resutured if violated. Finally, the alar cartilage is minimally disturbed, with preferences for suture techniques over excisional methods. In its purest form then, a preservation approach to rhinoplasty favors a closed approach. Although benefits of closed rhinoplasty can be theorized, there are significant benefits of open work. Moreso, many surgeons have elected to avoid or abandon preservation techniques, primarily because of poor results, less predictability, and complications (largely hump recurrence). The fusion of structural and preservation may alleviate some of these concerns.
Although more recent descriptions of this hybrid approach have emphasized preservation techniques for the dorsum (DPR) with lower third structural techniques, the integration of structure and preservation is more common when considering contemporary rhinoplasty. The authors here suggest several general categories to describe this integration. Each of these components may be exercised independently at the discretion of the rhinoplasty surgeon.
- 1.
DPR coupled with structural approaches to the lower third and the nasal tip
- 2.
Approaching structural lower-third manipulations with a preservation lens, such that there is limited resection of lower lateral cartilages with an emphasis on suture techniques
- 3.
In open nasal approaches, minimizing the degree of soft tissue disruption at the middle vault and dorsum when possible in structural and preservation cases
- 4.
Converting a nasal dorsum to a preservation candidate through the use of structural techniques, including osteoplasty, excision, or grafting (eg, radix, spreaders)
- 5.
Modified DPR techniques in which components of the nasal dorsum are treated with structural methodology or the ULCs are separated from the midline.
Dorsal preservation with structural approaches to the lower third
In patients with pleasing dorsal aesthetics on frontal view, the use of preservation techniques has been shown to yield positive patient-reported outcomes. , , Importantly, it should be noted that preservation techniques, based on current data, have not been shown to be superior to structural dorsal techniques. , , These positive outcomes are likely a product of good patient selection and technical execution, and highlight the need to understand the indications for preservation candidates. In addition, patient-reported outcome measures can miss granular details that may be better appreciated by rhinoplasty surgeons. In the authors’ experience, preservation methods for the dorsum yield an early favorable aesthetic and more predictable positive longer-term results. As such, there has been an emphasis on performing DPR when appropriate. However, preservation, particularly as it pertains to the dorsum, is not always feasible. An understanding of what scenarios will impart the greatest success using this ideology will prevent poor outcomes.
Preservation techniques are ideally performed in the setting of primary rhinoplasty. , In revision cases, there has been violation of the keystone, and there may be substantial structural deficiencies that are not amenable to preservation techniques. Patients with more kyphotic prominences, longer nasal bones (and analogously a shorter cartilaginous component to the dorsal hump), deep nasofrontal angles, wide or irregular nasal bones, and flared midvaults are less ideal candidates for DPR surgery, although these are not necessary absolute exclusion criteria. If the dorsum is not deemed to be of ideal shape or if the patient is unsatisfied with it on frontal view preoperatively, preservation surgery is less appropriate. As will be discussed later, there are methods to convert some of this anatomy to a state more favorable for preservation.
In SPR, the nose is widely decorticated in a supra-perichondrial subfascial plane. This transitions to a subperiosteal plane at the level of the nasal bones and affords wide exposure of the nasal tip, midvault, and bony pyramid. The requisites for dorsal lowering in an SPR approach include septal resection (cartilage ± bone) and separation of the osseous nasal pyramid from the surrounding bone. The latter may come in the form a push-down (PD) maneuver (lateral and root osteotomies with displacement of the bony vault into the nasal cavity medial to the maxilla) or a let-down (LD) maneuver (additional wedge resections at the nasal bones with the bony vault resting on the maxilla). The former has several variations categorized by location of septal excision (immediate subdorsal, subdorsal/intermediate, or low). , , , These techniques have been previously described and are not outlined in detail here. With subdorsal methods, cartilage that remains immediately below the dorsum can be more easily anchored to more inferior cartilage. In techniques where the caudal strut of cartilage is not violated (eg, in the modified subdorsal strip method [MSSM] or tetris method), the caudal septum can be utilized for tip stabilization. , The MSSM method has been favored by the authors, although other methods have been shown to have equally good results. In this method, a 5 to 7 mm subdorsal strut is preserved, as is a 1 to 1.5 cm caudal strut. The caudal septum can either be trimmed secondarily or left in its original location to allow for attachment of the tripod complex.
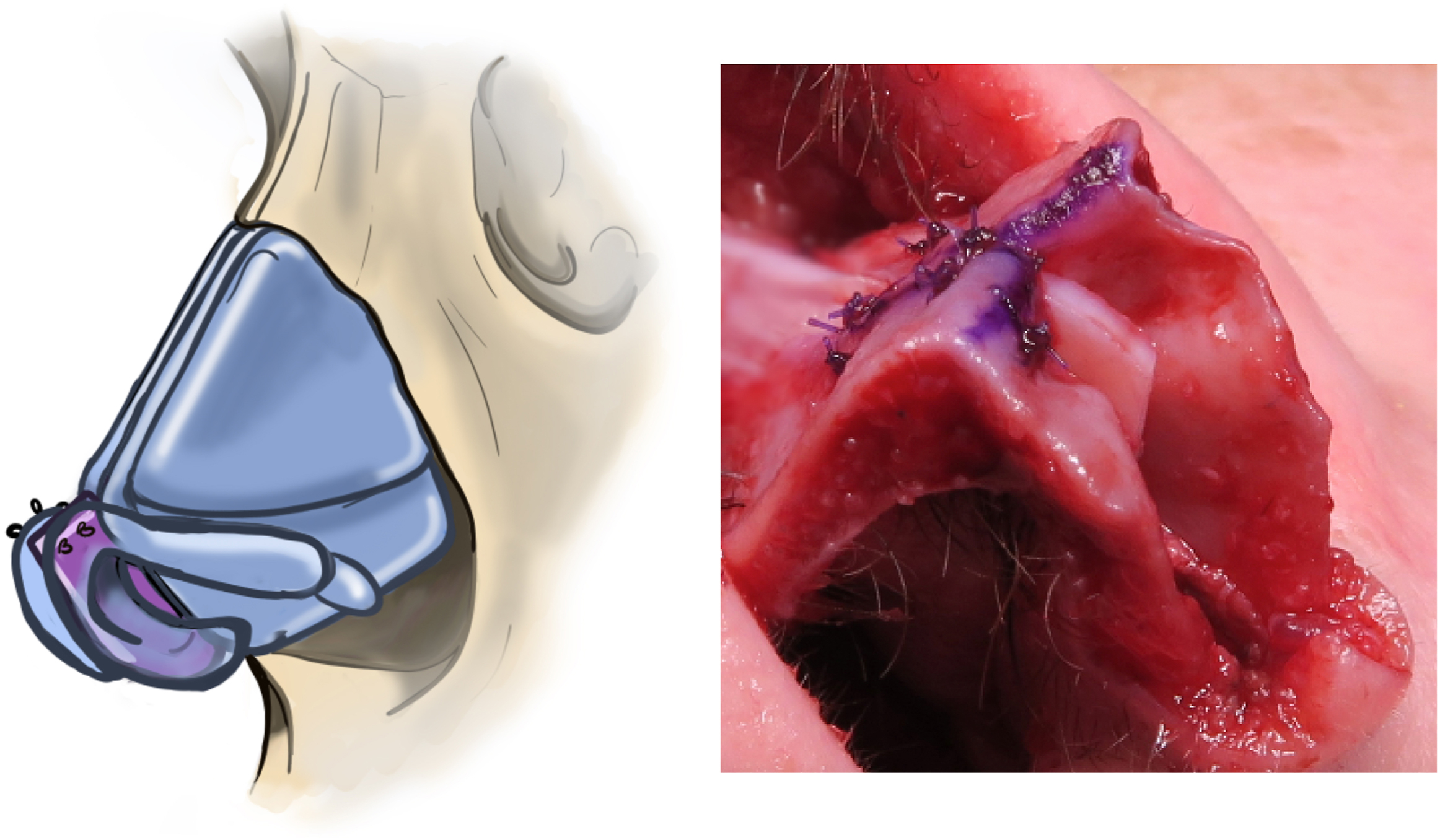
Manipulation of the dorsum via preservation methods is done before manipulation of the nasal tip. The nasal septum is also secured before finalizing changes to the lower third of the nose. Subsequently, additional maneuvers can be done to the caudal septum to either strengthen the caudal septal complex or extend it. In Cottle or SPAR techniques of managing the septum, the entire anterior septum can be repositioned to a newly desired position. However, repositioning and stabilizing the septum to the maxillary crest may be deemed a challenge. Nonetheless, this method can be powerful for anterior septal deformities. Grafts can be sutured to caudal portions of cartilage with most septal techniques. In the MSSM and tetris methods, grafts can be obtained from cartilage inferiorly, because this area has not been violated. In these methods, the preservation of a stable caudal septal segment also allows for the attachment of septal extension grafting ( Fig. 1 ). This is sutured anterior to the fusion site of ULC to the dorsal septum (W point). This grafting may impart additional stability to the septum, but also provides a more projected or rotated/counter-rotated position to anchor the nasal tripod. Notably, DPR techniques can place substantial downward force and torque on the caudal septum, causing unwanted deviation, and this should be carefully inspected. In some scenarios, the tripod can be sutured to the remaining caudal septum without extension, as it sits in a more superior position relative to the dorsum that has been lowered cephalically.
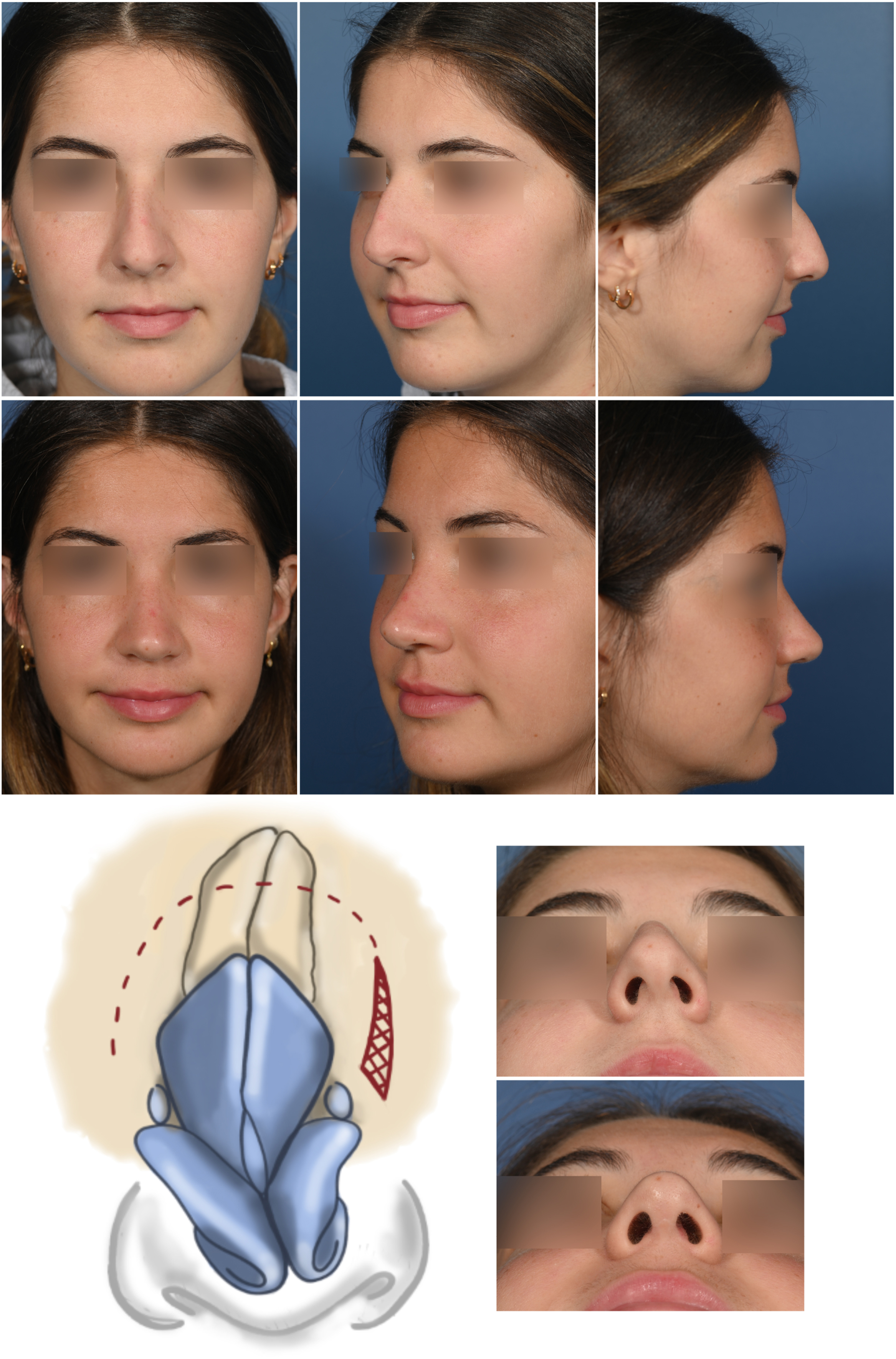
In the deviated nose, a asymmetric wedge resection of bone in an LD procedure with greater bone removed on the nondeviated side can help correct a straight deviation. , , Alternatively, the bone may only be resected on the side of the deviation, with a PD performed on the nondeviated side ( Fig. 2 ). These differential bony changes are stabilized by suturing the subdorsal septum to the lower septum on the nondeviated side. Although this will correct dorsal deviations, the nasal tip will need to be addressed via structural methods, a benefit afforded by SPR. A septal extension graft sutured to the preoperatively nondeviated side allows for stabilization of the nasal tip in a more midline orientation ( Fig. 3 ).

In cases with severe anterior septal deviations, the use of preservation techniques is less favorable. As aforementioned, the Cottle technique may be valuable in this setting. If necessary, an anterior septal reconstruction with resection of native caudal septum is possible with dorsal preservation. Use of the dorsal osseocartilaginous horizontal mattress (DOHM) suture is advantageous in this situation. Importantly, patients with dorsal humps and an associated high septal deviation may be best managed with preservation techniques. This is particularly true when the high septum deviates to the same side as the deviated nasal vault, a so-called unfavorable dorsal septal gap (DSG). This is because with traditional structural techniques, medialization of nasal bone on the deviated side after osteotomies will be hindered by the high septal deviation. ,
Finally, structural modification of the nasal tip can be performed in any capacity with traditional structural techniques. Although this topic is too exhaustive for review here, it should be noted that any traditional technique can be used for restructuring the ala cartilages. In cases of severely distorted lower lateral cartilages, partial resection and use of lateral crural strut grafting can be performed. This method also allows for repositioning of the ala. The use of miniature-lateral crural strut grafts can reduce the convexity of the ala and is an effective tip-plasty technique (3–4). These methods require elevation of the vestibular lining from the undersurface of the crura. Lateral crural overlay requires an incision of the lower lateral crura but can effectively deproject and rotate the tip. The overlap and preservation of, rather than resection of cartilage, minimizes weakness to the ala. The nasal tip can be suspended to the caudal septum or extension grafting with a tongue in groove or inter-domal/ala sutures (eg, alar spanning suture, figure of 8 suture through domes). Figs. 2–5 show examples of patients who have undergone structural preservation with preservation techniques used for the dorsum and structural techniques for the nasal tip.

Related posts:
 Understanding Dorsal Preservation Rhinoplasty
Understanding Dorsal Preservation Rhinoplasty
 Preservation Rhinoplasty—Outcomes in Dorsal Preservation Rhinoplasty
Preservation Rhinoplasty—Outcomes in Dorsal Preservation Rhinoplasty
 Subdorsal Flaps in Dorsal Preservation
Subdorsal Flaps in Dorsal Preservation
 Expanding Indications to Dorsal Preservation Rhinoplasty
Expanding Indications to Dorsal Preservation Rhinoplasty
 Spare Roof Technique A and B – A Step-by-step Guide to Avoid Suboptimal Outcomes
Spare Roof Technique A and B – A Step-by-step Guide to Avoid Suboptimal Outcomes
 Dorsal Augmentation with Preservation Concepts
Dorsal Augmentation with Preservation Concepts
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


