Columella and Nasal Septum Skin-Cartilage Flap to Nasal Ala
M. ORTICOCHEA
EDITORIAL COMMENT
This is an elegantly conceived procedure that is applicable to smaller defects, but there are several problems, including wound contraction and retraction, the possibility of producing asymmetry with the opposite side, the lack of color match, the unpredictability of the alar roll, and retraction of the columella.
Defects of the ala nasi are common, and many methods have been proposed for their repair. The following technique provides a repair of good shape, color, and texture and supplies sufficient cartilage to prevent the ala from collapsing during inhalation (1).
OPERATIVE TECHNIQUE
An anteriorly based flap is raised that consists of half the columella and the membranous septum, the medial crus of the alar cartilage, and as much of the skin lining from the cartilaginous septum as may be required (see Figs. 47.2 and 47.4). The medial crus of the alar cartilage is divided, producing a mobile flap that can be transposed readily and sutured into the alar defect.
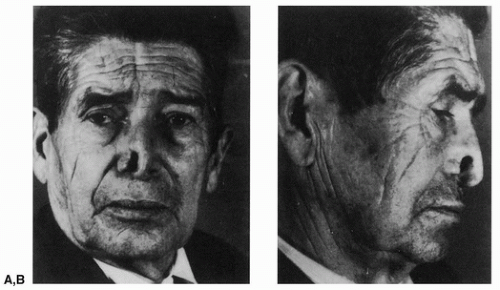 FIGURE 47.1 A,B: The alar defect. (From Orticochea, ref. 1, with permission.) |
The donor area is covered with a skin graft. The tissues are fairly stiff, and little deformation occurs. With smaller defects, the raw surface of the flap (inside the nostril) may be allowed to heal by secondary intention, and this may impart a natural roll to the reconstructed alar margin. With larger defects (Figs. 47.1, 47.2, 47.3, 47.4, 47.5), the flap as well as the donor area is skin-grafted.
Related posts:
 Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
 Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction
Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction
 Oral Mucosal Flaps for Septal Reconstruction
Oral Mucosal Flaps for Septal Reconstruction
 Postauricular and Retroauricular Scalping Flap (The Paras Flap)
Postauricular and Retroauricular Scalping Flap (The Paras Flap)
 Scapular and Parascapular Flaps
Scapular and Parascapular Flaps
 Platysma Musculocutaneous Flap to The Lower Lip
Platysma Musculocutaneous Flap to The Lower Lip
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


