Fig. 3.1
Classic examples of lentigo maligna (a) on the cheek in a 60 year old female, (b) on the nasal tip in an 83 year old male, (c) and on the scalp in a 78 year old male
Size
LM is slowly growing, asymptomatic and often occurs in the setting of mottled hyperpigmentation. By the time they are biopsied, they are often larger in size (Fig. 3.2). In a retrospective study by Tiodorovic-Zivkovic et al., 48.8 % of lesions were > 10 mm in diameter at the time of biopsy. Similarly, 49.3 % of LMs biopsied had surrounding freckles, reinforcing the concept that these lesions arise in chronically sun-damaged skin (Fig. 3.3) [3].


Fig. 3.2
2.5 cm lentigo maligna lesion on forehead
Fig. 3.3
Biopsy proven lentigo maligna surrounded by chronically sun-damaged skin on the (a) neck and (b) arm
Morphology (Borders and Colors)
Most LMs present as asymmetric brown-black macules or patches with variegated color and irregular borders [4]. The differential diagnosis includes solar lentigo, seborrheic keratosis (Fig. 3.4), lichenoid keratosis, pigmented actinic keratosis, and melanocytic nevus. In a study of 121 melanoma in situ lesions, 92 % were macular. In that same study, 75 % of the melanoma in situ lesions had asymmetric borders [4]. In a study of 186 melanomas of various subtypes (LM, superficial spreading melanoma, desmoplastic melanoma, and nevoid melanoma), light-and dark-brown were the most frequently seen colors [n = 161 (86.6 %) and n = 158 (84.9 %), respectively]. Pink was appreciated in 56 cases (30 %) while white was seen in 10 cases (5.4 %). Melanoma in situ most commonly demonstrated 2 colors [n = 97 (68.3 %)] while 9.9 % showed only 1 color and 21.8 % showed 3+ colors [5]. Infrequently it is even possible for LM/LMM to have an amelanotic presentation as depicted in Fig. 3.5.


Fig. 3.4
Clinical example of (a) solar lentigo and (b) seborrheic keratosis
Fig. 3.5
Amelanotic lentigo maligna melanoma
ABCDE’s of Melanoma
In the early 1980s, a group of dermatologists created an algorithm for detecting melanomas based on their experience at NYU. At that time, melanoma detection was emphasized by Asymmetry, Border irregularity, and Color variegation [6]. This mnemonic has since been expanded to include Diameter greater than 6 mm and Evolution (lesions changing over time). The mnemonic ABCDEs of melanoma is commonly used by many physicians to raise melanoma awareness and educate the public about those lesions that may call for further evaluation. While this mnemonic can be used in evaluating lesions of LM/LMM, simply failing to notice which lesion to evaluate contributes to the delay in diagnosis. Most lesions of LM/LMM occur on the face and are plainly in view. Many have been followed for years by physicians and patients. The often larger size and longer duration before diagnosis speaks to their slow, stealthy growth, asymptomatic nature and camouflaged appearance against a background of photo damage (Fig. 3.6). These characteristics contribute to delay in diagnosis and highlight the need for the practitioner to maintain a high level of vigilance and suspicion, to sometimes step back and evaluate the patient’s skin globally and to notice pattern rather than individual lesion as stressed by the ABCDE mnemonic.

Fig. 3.6
Biopsy proven lentigo maligna on the cheek (circled) surrounded by sun damaged skin
Deciding Whether and How to Biopsy
As above, LMs are slowly growing and often asymptomatic. They typically occur in patients who may have decreased vision and therefore identification of suspicious lesions often relies on the physician’s experience and level of suspicion. Clinicians seeing elderly fair skinned patients must remain vigilant and must carry a high index of suspicion and a low threshold for biopsy. A dermatoscope and/or a Wood’s lamp may aid the clinician in the decision to biopsy but given the degree of clinical overlap, definitive diagnosis often relies on histopathologic examination.
Wood’s Lamp
The Wood’s lamp consists of a mercury vapor light source with a filter, which emits wavelengths from 320 to 450 nm, with peak emission at 365 nm. Epidermal melanin absorbs the shorter wavelengths emitted from the Wood’s lamp, making superficially pigmented lesions appear darker than the surrounding normal epidermis (Fig. 3.7a). Superficially pigmented lesions can be more easily visualized and outlined with the Wood’s lamp. However, a clinician must recognize that dermal melanin is not accentuated by the Wood’s light and may lead to false reassurance regarding a deeper atypical melanocytic lesion, such as a metastatic melanoma deposit or primary dermal melanoma [7]. Many benign melanocytic lesions are highlighted by the Wood’s lamp including ephelides, lentigines, and nevi, and in the setting of diffuse photodamage this sometimes limits its utility as a diagnostic tool (Fig. 3.7b). For these reasons and in the authors’ experience, the Wood’s lamp may be more useful in helping the clinician estimate the size of lesions of LM with subclinical disease (i.e. lesion that may not be apparent to the naked eye) rather than in diagnosis (Fig. 3.7c).
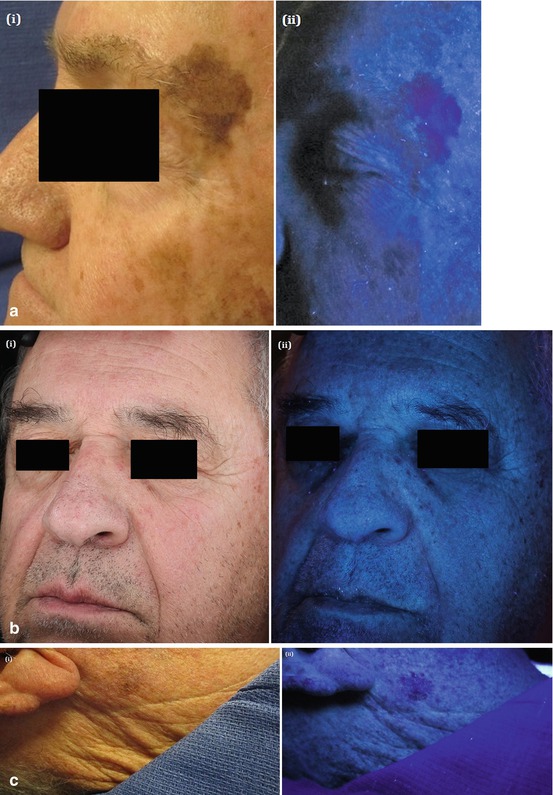
Fig. 3.7
 Epidemiology and Natural History
Epidemiology and Natural History
 Incorporating Patient Preferences and Quality of Life
Incorporating Patient Preferences and Quality of Life
 Case B: Unsuspected Invasion and Upstaging in Lentigo Maligna Melanoma
Case B: Unsuspected Invasion and Upstaging in Lentigo Maligna Melanoma
 Staged Excision Techniques
Staged Excision Techniques
 Follow Up and Recurrence
Follow Up and Recurrence
 Case A: Multiple Mapping Techniques to Guide Staged Excision for a Challenging Lentigo Maligna Melanoma
Case A: Multiple Mapping Techniques to Guide Staged Excision for a Challenging Lentigo Maligna Melanoma




(a) (i) Pigmented lesion on lateral brow (ii) Wood’s lamp accentuating pigmentation. (b) (i) Patient with extensive photodamage (ii) Wood’s lamp highlighting multiple benign pigmented lesions. (c) (i) Pigmented lesion below right ear (ii) Wood’s lamp helping to estimate lesion size
Related posts:
Epidemiology and Natural History
Incorporating Patient Preferences and Quality of Life
Case B: Unsuspected Invasion and Upstaging in Lentigo Maligna Melanoma
Staged Excision Techniques
Follow Up and Recurrence
Case A: Multiple Mapping Techniques to Guide Staged Excision for a Challenging Lentigo Maligna Melanoma
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
