Traumatic nerve injuries are common conditions treated by hand surgeons, and the optimal treatment of a severed nerve requires providing a healthy wound bed, generous trimming to healthy nerve substance, and a minimal-tension approximation. The gold standard for repair of a critical nerve gap has been the nerve autograft. However, results are generally less favorable than direct suture. Autogenous and synthetic conduits and processed nerve allografts have been developed as less morbid and more convenient alternatives to autografts, but the reported outcomes have been uneven. Engineered neural tissues show great promise in inducing nerve regeneration across a gap.
Key points
- •
The optimal repair of a nerve with a critical gap remains an important unanswered question in hand surgery.
- •
Autografts have long been the “gold standard” for nerve gap repair, but results are less favorable than direct suture, and a donor site is required.
- •
Synthetic and biologic conduits have a long history and seem to be effective for short gaps in sensory nerves.
- •
Processed nerve allografts have rapidly gained popularity and early functional outcomes are promising, especially for sensory nerves.
- •
Engineered neural tissues show great promise in inducing nerve regeneration across a gap in preclinical studies.
Introduction
Traumatic nerve injuries are among the most common conditions treated by hand surgeons. These injuries can be encountered in isolation or as one component of a complex injury pattern. In the patient with a complex mangling hand injury, the quality of sensory and motor recovery is often the most important factor determining outcome. The practicing hand surgeon must be familiar with the biology of nerve regeneration, the principles of microsurgical nerve repair, and the factors that influence recovery.
Nerve regeneration is a complex process involving the injured neurons, Schwann cells, satellite or glial cells, and macrophages and other inflammatory cells. From the moment of injury, signals are sent from the site of injury to the cell body, which initiates the process of regeneration. Inflammatory mediators are liberated at the injury site, which recruit macrophages, phagocytes, and Schwann cells. The axon sprouts and a growth cone is formed at the tip of each sprout, which interacts with the activated and proliferating Schwann cells. The directionality of the outgrowing axon is determined by a complex interplay of Schwann cell and axonal factors. This sequence of events describes the ideal scenario, but nerve injury in the clinical setting is rarely ideal. The presence of devitalized tissue, hematoma, or bacterial contamination impairs the process of regeneration. In a traumatic wound with a level V nerve injury (neurotmesis), the physiologic response to injury involves fibroblast recruitment and collagen deposition in the nerve gap, precluding regeneration. Functional recovery following a level V injury requires operative intervention.
The principles of successful nerve repair have changed little since their description by Ferrara in the sixteenth century and consist of generous trimming of the nerve to healthy substance, minimal-tension approximation, and providing a well-vascularized wound bed. However, it is seldom possible to provide a tension-free approximation, especially in the setting of crush or avulsion mechanisms with a wide zone of injury. In general, a primary repair is preferable to bridging a gap with a graft. Animal studies have shown that a percentage of the total nerve fibers are lost at every surgical coaptation site. However, tension at the repair site has also been shown to impair regeneration, likely because of its effect on microvascular flow. Clinical judgment must be used to determine when a primary repair is preferred or not. The oft cited 9-0 nylon test is helpful, whereby if the nerve can be reapproximated with a single 9-0 nylon suture, without breakage, then primary repair is performed. According to Lohmeyer and colleagues, using this criterion, direct repair is not possible in 18% of digital nerve injuries.
Despite the prevalence of nerve injuries in the hand, and a large body of literature on the subject, no consensus exists as to the optimal management of a nerve injury with a critical gap. This review surveys the full range of nerve gap repair techniques ( Box 1 ), including autograft, conduits, processed allograft, and engineered neural tissue, to critically appraise the current evidence for each and to propose a rational treatment algorithm.
Principles of Successful Nerve Repair
- •
Adequate lighting and magnification
- •
Generous trimming of nerve to healthy-appearing axons
- •
Minimal tension approximation
- •
Fine monofilament suture, as few as possible
- •
Proper alignment of fascicles
| Repair Technique | Pros | Cons |
|---|---|---|
| Autograft | Inexpensive | Donor morbidity |
| Biocompatible | Longer operative time | |
| More reliable | Limited available length | |
| Delivers Schwann cells | ||
| Processed allograft | Readily available | Expensive |
| Technically easy and quick | No Schwann cells | |
| Well tolerated | Patients may object to cadaveric tissue | |
| No donor site | ||
| Synthetic conduit | Readily available | Expensive |
| Technically easy | No Schwann cells | |
| No donor site | May extrude | |
| Vein conduit | Inexpensive | Donor site scar |
| Biocompatible | Longer operative time | |
| May collapse | ||
Introduction
Traumatic nerve injuries are among the most common conditions treated by hand surgeons. These injuries can be encountered in isolation or as one component of a complex injury pattern. In the patient with a complex mangling hand injury, the quality of sensory and motor recovery is often the most important factor determining outcome. The practicing hand surgeon must be familiar with the biology of nerve regeneration, the principles of microsurgical nerve repair, and the factors that influence recovery.
Nerve regeneration is a complex process involving the injured neurons, Schwann cells, satellite or glial cells, and macrophages and other inflammatory cells. From the moment of injury, signals are sent from the site of injury to the cell body, which initiates the process of regeneration. Inflammatory mediators are liberated at the injury site, which recruit macrophages, phagocytes, and Schwann cells. The axon sprouts and a growth cone is formed at the tip of each sprout, which interacts with the activated and proliferating Schwann cells. The directionality of the outgrowing axon is determined by a complex interplay of Schwann cell and axonal factors. This sequence of events describes the ideal scenario, but nerve injury in the clinical setting is rarely ideal. The presence of devitalized tissue, hematoma, or bacterial contamination impairs the process of regeneration. In a traumatic wound with a level V nerve injury (neurotmesis), the physiologic response to injury involves fibroblast recruitment and collagen deposition in the nerve gap, precluding regeneration. Functional recovery following a level V injury requires operative intervention.
The principles of successful nerve repair have changed little since their description by Ferrara in the sixteenth century and consist of generous trimming of the nerve to healthy substance, minimal-tension approximation, and providing a well-vascularized wound bed. However, it is seldom possible to provide a tension-free approximation, especially in the setting of crush or avulsion mechanisms with a wide zone of injury. In general, a primary repair is preferable to bridging a gap with a graft. Animal studies have shown that a percentage of the total nerve fibers are lost at every surgical coaptation site. However, tension at the repair site has also been shown to impair regeneration, likely because of its effect on microvascular flow. Clinical judgment must be used to determine when a primary repair is preferred or not. The oft cited 9-0 nylon test is helpful, whereby if the nerve can be reapproximated with a single 9-0 nylon suture, without breakage, then primary repair is performed. According to Lohmeyer and colleagues, using this criterion, direct repair is not possible in 18% of digital nerve injuries.
Despite the prevalence of nerve injuries in the hand, and a large body of literature on the subject, no consensus exists as to the optimal management of a nerve injury with a critical gap. This review surveys the full range of nerve gap repair techniques ( Box 1 ), including autograft, conduits, processed allograft, and engineered neural tissue, to critically appraise the current evidence for each and to propose a rational treatment algorithm.
Principles of Successful Nerve Repair
- •
Adequate lighting and magnification
- •
Generous trimming of nerve to healthy-appearing axons
- •
Minimal tension approximation
- •
Fine monofilament suture, as few as possible
- •
Proper alignment of fascicles
| Repair Technique | Pros | Cons |
|---|---|---|
| Autograft | Inexpensive | Donor morbidity |
| Biocompatible | Longer operative time | |
| More reliable | Limited available length | |
| Delivers Schwann cells | ||
| Processed allograft | Readily available | Expensive |
| Technically easy and quick | No Schwann cells | |
| Well tolerated | Patients may object to cadaveric tissue | |
| No donor site | ||
| Synthetic conduit | Readily available | Expensive |
| Technically easy | No Schwann cells | |
| No donor site | May extrude | |
| Vein conduit | Inexpensive | Donor site scar |
| Biocompatible | Longer operative time | |
| May collapse | ||
Autografts
The first experimental work on nerve grafting was performed in 1869, when Philippeux and Vulpian reported a remarkable series of experiments on the lingual and hypoglossal nerves in a canine model and noted that distal regeneration can occur. The landmark work of Huber and Bunnell established nerve autografting as a clinical reality, and by the 1940s, nerve autografts had become the standard repair technique when primary suture was not possible.
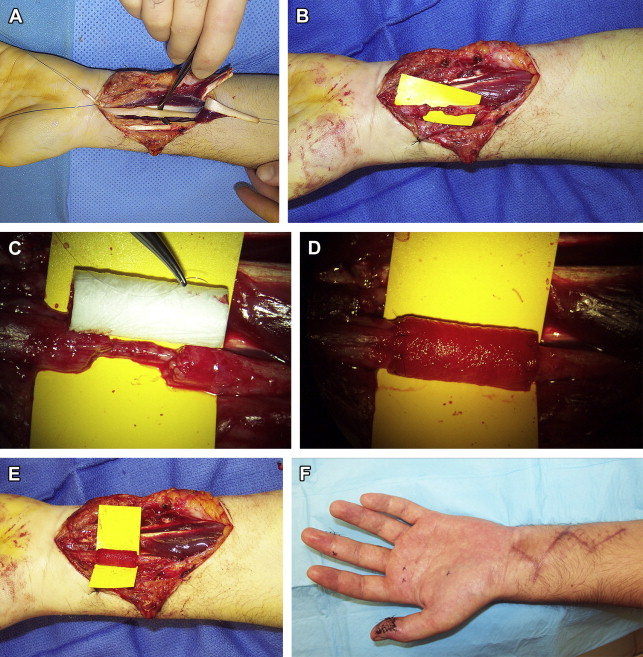
Nerve autografts are biocompatible, readily available, and inexpensive. They provide a stimulating scaffold, including viable Schwann cells and neurotrophic factors, which have been shown experimentally to play an important role in supporting regenerating axons. This scaffold seems to be especially important in bridging long nerve gaps. The major disadvantages of autografting include the increased operating time and complexity associated with nerve harvest, a second surgical wound, and donor site nerve deficits. Donor sites can rarely be associated with significant and long-standing morbidity, including anesthesia, paresthesias, and pain. Many options for donor nerves have been described for upper extremity reconstruction, with the sural nerve, the lateral antebrachial cutaneous nerve, and the anterior division of the medial antebrachial cutaneous nerve being popular choices. To determine the appropriate donor nerve, the surgeon must consider the caliber of the nerve to be repaired, the length of the defect, and donor site morbidity. The terminal branch of the posterior interosseous nerve (PIN), which can be found in the volar aspect of the fourth dorsal extensor compartment, is a good caliber match for a distal digital nerve, and can be harvested with little or no donor site deficit ( Fig. 1 ). Nerve autografts should be reversed in orientation, to avoid loss of axons through small side branches of the nerve.

There are several well-designed retrospective series that have reported outcomes following digital nerve reconstruction with autografts in the clinical setting. Nunley and colleagues, in 1989, published a series of 21 digital nerve gaps repaired with medial antebrachial cutaneous nerve autografts. Recovery of at least 15 mm 2-point discrimination was reported in 86% of patients, all of whom had a gap length of 1 to 2 cm. Two years later, Frykman and Gramyk reported recovery to at least the S3+ level on the Medical Research Council Classification Scale ( Table 1 ) in 95% of 73 patients with digital nerve gaps treated with autografting. Patients with gap lengths up to 3 cm were included. In 1993, Kallio presented the results of a series of 254 digital nerve repairs in 95 patients, the largest of its kind to date. Thirty-seven patients were treated with nerve autografts, with gap lengths up to 5 cm. Useful sensory function, defined as S3 or greater recovery, was observed in 56% of patients in the autograft subset, compared with 80% in the direct suture group. A recent meta-analysis pooled data from all existing retrospective studies on digital nerve repair. Data from 18 studies on autograft reconstruction were pooled, including 384 nerve grafts with at least 1-year follow-up and sufficiently complete outcomes measurements. The proportion of patients with at least an S3+ level of recovery after autografting was 67%.
| Sensory | ||||
|---|---|---|---|---|
| Outcome | Classification | s2PD (mm) | m2PD (mm) | Recovery of Sensibility |
| Failure | S0 | — | — | No recovery of sensibility in the autonomous zone of the nerve |
| Poor | S1 | — | — | Recovery of deep cutaneous pain sensibility in the autonomous zone of the nerve |
| S1+ | — | — | Recovery of superficial pain sensibility | |
| S2 | — | — | Recovery of superficial pain and some touch sensibility | |
| S2+ | — | — | As in S2, but with overresponse | |
| S3 | >15 | >7 | Recovery of pain and touch sensibility with disappearance of overresponse | |
| Good | S3+ | 7–15 | 4–7 | As in S3, but with good localization of the stimulus and imperfect recovery of 2PD |
| Excellent | S4 | 2–6 | 2–3 | Complete sensory recovery |
| Motor | ||
|---|---|---|
| Outcome | Classification | Findings |
| Failure | M0 | No evidence of contractility |
| Trace | M1 | Evidence of slight contractility. No joint motion |
| M1+ | Proximal muscles contract against gravity but distal muscles are paralyzed | |
| Poor | M2 | Complete range of motion with gravity eliminated |
| M2+ | Proximal and distal muscles are active against gravity | |
| Fair | M3 | Complete range of motion against gravity |
| Good | M4 | Complete range of motion against gravity with some resistance |
| Excellent | M5 | Complete range of motion with full resistance |
Forearm injuries involving the median or ulnar nerves are common injuries with profound functional implications. As these are mixed nerves with sensory and motor components, the precise identification and orientation of fascicles is a key component in their successful repair. A delay in ulnar or median nerve repair has been shown to have a negative impact on outcome, an observation that may be due to the difficulty in orienting fascicles after a delay with resulting intraneural scarring. For this reason, the protocol at our institution is to repair median or ulnar nerves within 24 hours of injury.
There have been several large retrospective series of median and ulnar nerve repairs with autografts. One of the largest series of nerve injuries was published by Secer and colleagues in 2008, consisting of 2210 military-related peripheral nerve injuries. Their series included 159 median and ulnar nerves treated with autografting, of which M3 or better motor recovery was seen in 61% of median and 58% of ulnar nerve repairs. S3 or better sensory recovery was seen in 76% of median and 65% of ulnar nerves. In a recent meta-analysis of ulnar and median nerve reconstructions pooling data from 1531 nerve repairs, meaningful recovery was observed in 49% of patients undergoing reconstruction with autografts for gap lengths of 5 cm or less. This result was not statistically different from the results for conduit reconstruction.
Synthetic conduits
The concept of bridging a peripheral nerve gap with a hollow conduit is not new. In the 1890s, Büngner bridged a canine sciatic nerve gap with a segment of human brachial artery. During the ensuing decades, nerve conduits composed of many materials were explored, including gelatin, agar, bone, metal, and rubber, with variable clinical success. Nonbiodegradable conduits have since fallen out of favor, but resorbable conduits made from polyglycolic acid, aliphatic polyesters and copolyesters, and purified bovine type I collagen remain in use. The most conspicuous advantage of nerve conduits is that they obviate a nerve donor site and the associated morbidity. In addition, allowing a severed nerve ending to grow across a confined gap allows growth factors to influence the proximal growth cone. In experimental models, this has been shown to result in more accurate alignment of nerve endings ( Fig. 2 ). However, conduits add expense to nerve reconstruction, and they lack laminin scaffolding and Schwann cells, which play a vital role in supporting axonal regeneration, especially over longer gaps. They also add a foreign body burden to a wound, which may have bacterial contamination or vascular compromise, and extrusions have been reported.
The rates of recovery for conduit repairs of digital nerves have varied widely in published reports, but have been comparable to autograft for short gaps. In a multicenter prospective study, Weber and colleagues reported a meaningful recovery rate of 74% in 56 digital nerve repairs using woven polyglycolic acid (PGA) conduits with a gap length of less than 25 mm. Battiston and colleagues, also using PGA conduits, reported recovery to the S3+ level in 69% of 19 patients with gap lengths of 1 to 4 cm (mean 2 cm). Better results have been reported in 2 more small retrospective studies evaluating collagen conduits in digital nerve repair. Bushnell and colleagues, in 2008, reported 100% recovery to the S3+ level in 9 patients with gap lengths less than 2 cm, and Thomsen and colleagues reported a 92% recovery in 11 patients with gap lengths between 1 and 2 cm following resection of digital neuromas. A recent meta-analysis pooled data from 6 studies on digital nerve repair with synthetic conduits. The proportion of patients with at least an S3+ level of recovery after conduit repair was 79%, which did not differ significantly from autograft repair. Further analysis confirmed that recovery rates deteriorated with gap lengths measuring more than 3 cm. These results suggest that PGA and collagen conduits are as effective as autografts for sensory gaps 20 mm or less, but it is still unclear whether synthetic conduits are beneficial for longer gaps.
Conduits made of poly ( dl -lactide-ε-caprolactone) (PCL) have become commercially available. PCL conduits are transparent and resorb through hydrolysis with a less acidic degradation product than PGA. In a randomized prospective multicenter trial, PCL conduits were shown to be as effective as autograft in 3 groups stratified by gap length. However, subsequent studies have been less favorable. Chiriac and colleagues reported a series of 28 upper extremity nerve repairs with PCL conduits and reported a 25% meaningful recovery rate and a 35% complication rate. In light of these conflicting data, the effectiveness of PCL conduits remains unclear.
There are several retrospective series of median and ulnar nerve reconstruction using nonresorbable (silicone or Polytetrafluoroethylene [pTFE]) conduits, with good recovery reported. For resorbable conduits, the literature consists largely of isolated case reports and small clinical series ( Fig. 3 ). Due to the paucity of data, it is impossible at this time to render a verdict regarding the relative effectiveness of conduits versus autograft for reconstruction of mixed nerves in the forearm.