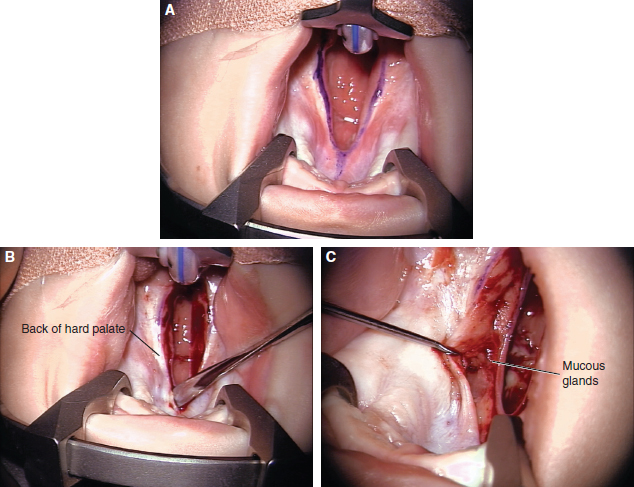
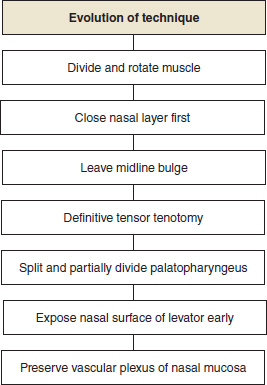
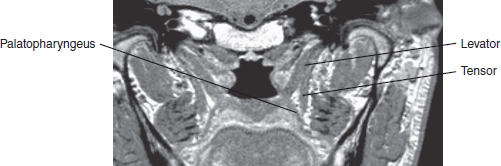
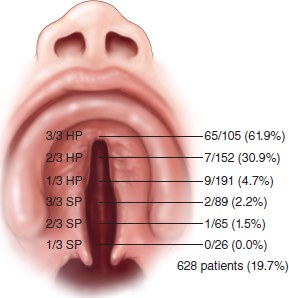
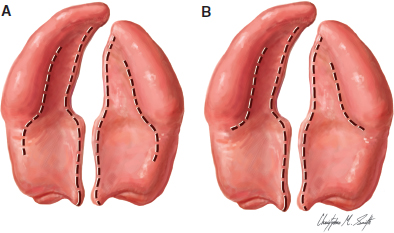
50 ○ Cleft palate repair is the most important component of cleft surgery, because it determines the speech and communication outcome and potentially has the greatest effect on maxillary growth and dental arch relationship and probably also on hearing. ○ Some cleft palates (particularly in certain syndromes) are undoubtedly hypoplastic. However, all cleft palates have abnormal anterior insertion of the palate muscles, particularly the levator veli palatini (the levator). ○ The term intravelar veloplasty has been used to describe an attempt to correct the muscle abnormality. However, this means different things to different surgeons. ○ The technique involving dissection between the oral mucosa and muscle and between the nasal mucosa and muscle and then retropositioning and reconstruction of the palate muscles. This is best done using an operating microscope. ○ Wherever possible, the palate should be closed without lateral releasing incisions. Whether this is possible depends on the type, extent, and width of the cleft. ○ Speech assessment is the prime outcome measure, but it is very difficult to compare between centers because of the lack of consensus criteria among countries and across languages. Ideally, speech should be blindly assessed by external speech pathologists. ○ Both the eventual outcome and the burden borne by patient and parents to achieve this outcome need to be considered. Cleft palate repair is the most important component of cleft surgery; it determines the patient’s speech and communication outcome and potentially has the greatest effect on maxillary growth and dental arch relationship.1 The primary aims of cleft palate repair are to improve feeding, to achieve normal speech, and to minimize adverse effects on maxillary growth. The technique of palate repair may also have an effect on middle-ear function and hearing. Victor Veau2 described the abnormal palatal muscle anatomy in a cleft palate. From his observations, Veau concluded that speech outcomes could be improved by early palate repair. Braithwaite3 and later Kriens4 proposed surgical techniques to correct the abnormal anatomy of the velar musculature. Others believed that velar function could be improved by palatal pushback.5–7 However, evidence now suggests that push-back techniques are damaging to maxillary growth.1,8 My technique, as described here, began in 1974 with attempts to manage patients who had velopharyngeal dysfunction after palate repair by rerepair with muscle dissection and reconstruction, rather than through the use of traditional pharyngeal flaps or pharyngoplasties. Evidence of improvement in palate function after rerepair encouraged attempts to correct the muscle malposition in primary cleft palate repair.9,10 The technique has evolved over 40 years (Fig. 50-1). Fig. 50-1 The evolution of a cleft palate repair technique. Each of these developments has made the procedure more precise and easier to perform. The technique was first reported after 25 years of evolution.11 Whenever possible, the procedure should be carried out under an operating microscope, which greatly improves visualization of the anatomy and increases the safety and reliability of the operation.12 Because of the long learning curve and potential for doing significant harm, this procedure is not appropriate for the occasional operator. Rates of velopharyngeal dysfunction after palatal repair have been reported to range from 4% to 70%. Differences in reporting protocols make such figures unreliable. However, no technique will produce a velopharyngeal mechanism that is competent throughout life in every patient; the palate is short in many patients with clefts.13 The palatal tissues (particularly in patients with certain syndromes) are undoubtedly hypoplastic. All cleft palates have abnormal insertion of the palatal muscles, particularly the levator veli palatini (the levator). This muscle is always oriented sagittally in patients with palatal clefts and inserts abnormally into the cleft margin in the anterior half of the velum. The levator itself does not insert into the back of the hard palate, as commonly described. The term intravelar veloplasty has been used to describe surgical procedures that attempt to correct the muscle abnormality.4 However, this term means different things to different surgeons.14 My technique involves dissection between the oral mucosa and muscle and between the nasal mucosa and muscle, then retropositioning and reconstructing the palatal musculature. Cutting et al15 independently developed a technique that bears some similarities to that described here, but with several major differences. An ingenious alternative approach to correct the muscle abnormality is the double-opposing Z-plasty technique described by Furlow,16 wherein the muscles are retrodisplaced, attached on one side to the oral mucosa and on the other side to the nasal mucosa. This procedure has the theoretical advantage of also lengthening the soft palate by narrowing it, because it has to expand transversely as well as longitudinally with elevation. The Furlow palatoplasty is an asymmetrical procedure, and asymmetry of function has been observed (P. Chen, personal communication, 2011). Despite this, the procedure has many strong advocates. However, the Furlow technique may be difficult to perform in wide clefts and is difficult to revise. Very satisfactory results have been reported by many surgeons. However, good comparative data, comparing this approach to radical muscle correction are not available. The technique is described in detail in Chapter 49. I have used the technique described in this chapter for virtually all patients undergoing palate repair. The only exception is the very uncommon patient with such a wide cleft that safe muscle reconstruction is not possible, in whom preliminary soft palate adhesion is carried out. The literature offers considerable support for the concept that palate repair (at least repair of the soft palate) should be performed before 12 months of age, and evidence from a randomized controlled trial suggests that speech outcome is better if the palate is repaired at 6 months of age rather than 12 months.17,18 In the latter study, the children with clefts repaired at 6 months of age did not develop compensatory articulation, whereas there was an incidence of compensatory articulation in those repaired at 12 months. Repair before significant babbling commences provides the best environment for early acquisition of consonants and speech development and also improves feeding, so I try to perform cleft palate repair at the age of 6 months. The major argument against early closure is the possible effect of early hard palate surgery on maxillary growth.19 An ongoing study in the United Kingdom, Scandinavia, and Brazil (the Timing of Primary Surgery for Cleft Palate [TOPS] trial) will compare the results of palate closure at 6 and 12 months, with the surgeons performing the technique presented here, to help elucidate the ideal timing. Evidence from countries where patients often present late with unrepaired cleft palates suggests that palate repair after the age of 8 to 12 years is unlikely to produce acceptable speech, especially if speech therapy is not available.19,20 Nevertheless, late closure of the hard palate in such patients may still be indicated for social and psychological reasons. Separating the nasal and oral cavities should be beneficial for eating and swallowing. A taskforce commissioned for the 2013 International Congress on Cleft Lip and Palate and Related Craniofacial Anomalies has published its report with recommendations and areas in which new or additional research is needed.21 Above all else, safe cleft palate surgery (particularly in young infants) requires high-quality pediatric anesthesia and postoperative care. Preoperative assessment should ensure that the patient is not anemic and not significantly underweight, although infants with cleft palate tend to be below the average of weight for age. The airway should also be assessed, because palate repair may, at least temporarily, compromise the upper airway. The general anesthetic should be administered in such a way that the airway is preserved, allowing the surgeon access to the palate. Intravenous access is secured for drug administration, fluid administration, and, rarely, blood replacement. An operating microscope should be used for the palate repair.12 The advantages of the microscope are: • The microscope provides high-quality variable magnification and good lighting directed at the operating field. It is therefore much more reliable than the alternative of magnifying loupes and a headlight. Improvements in visualization have led to refinements of palate repair and palate rerepair. • By frequently changing the tilt of the binoculars, the surgeon is able to sit in a relatively comfortable position throughout the entire procedure. • Magnification can be varied, “zooming in” for more detailed parts of the dissection. • The assistant obtains an excellent view through the side teaching arm and quickly learns to cut sutures and assist through this side view. He or she may also view the video monitor. The opportunity to demonstrate the operation to the operating room nurses greatly increases their involvement in the procedure and makes it possible to demonstrate palate surgery adequately to trainees and visitors. Both the assistant and those viewing the video monitor have the same view as the surgeon. • Still photograph or video records of the repair can be obtained. Using the microscope requires a period of adjustment and acclimation, but the advantages soon become apparent. The ideal requirements for the operating microscope for cleft palate repair are fairly basic: • Focal length variable or 250 to 300 mm • Adjustable angle of binoculars Fig. 50-2 A modified mouth gag for cleft palate repair. • Sideways rotation • Side arm for assistant • Side arm for video (if for demonstration) If a microscope is not available, 3.5× magnifying loupes with an attached headlight can be used, but this is a compromise that makes the soft palate muscular dissection and reconstruction less safe. A modification of the Dott-Kilner version of the Boyle Davis gag facilitates repair under the operating microscope and helps to prevent compression of the orotracheal tube on the mandible22 (Fig. 50-2). Other surgeons prefer the Dingman gag, which uses lateral traction of the cheek. Surgeons vary in their preferences for instruments. A Beaver knife with a No. 69 blade is very useful for incisions at the cleft margin and for commencement of mobilization of the oral mucoperiosteal flaps. Although anatomy is discussed elsewhere in this book (Chapter 6), certain aspects are of particular relevance to this repair technique. The oral mucoperiosteum of the hard palate receives its neurovascular supply from the greater palatine vessels and nerves, which emerge through the greater palatine foramina in the posterolateral corners of the hard palate. Multiple branches pass anteriorly, medially toward the cleft margin, and laterally to the alveolus. The latter may be divided when lateral releasing incisions are made. The nasal layer of the hard palate is continuous laterally with the lateral nasal wall. In a unilateral cleft lip and palate, the nasal layer is formed medially from vomerine mucosa. In a bilateral cleft or an isolated cleft palate involving the hard palate, the vomer is in the midline and not in continuity with the palatal shelves. In a normal palate, the levator muscle reaches the midline in the middle 40% of the velum.23,24 In a cleft palate, the levator passes from its origin at the skull base, downward and medially, to insert into the cleft margin in the anterior half of the velum (but not directly into the back of the hard palate, as is often stated). The palatopharyngeus muscle arises from the soft palate. Its larger component passes downward in the posterior pillar of the fauces to insert into the thyroid cartilage. Its smaller nasal component lies on the nasal side of the levator and passes around the pharynx to the posterior midline. It is believed to create Passavant’s ridge. Fig. 50-3 MRI in the plane of the levator at 60 degrees from the horizontal. In the soft palate, the palatopharyngeus and palatoglossus lie mainly on the oral side of the levator. The palatopharyngeus fans out from the fauces with some fibers passing forward toward the region of the maxillary tuberosity and pterygoid hamulus, and other fibers passing more medially toward the cleft margin (in its anterior two thirds to three quarters) and toward the back of the hard palate. The levator passes upward and backward to its origin, whereas the palatopharyngeus and palatoglossus pass downward and backward toward their insertions. They are, therefore, closely related near the midline but diverge laterally. Retrodisplacing the muscle that is attached to the back of the hard palate (the palatopharyngeus) but leaving the levator anteriorly inserted on the nasal layer is possible but defeats the object. The tensor veli palatini muscle passes from the skull base to the pterygoid hamulus, to which, in the cleft palate, its tendon partially attaches and appears to diverge into two components: (1) a nasal component that is a triangular tendinous insertion into the lateral part of the posterior border of the hard palate, where it lies adjacent to the nasal mucosa, and (2) a less robust component that passes orally toward the oral mucosa. This component is seen during techniques that involve lateral releasing incisions for relief of tension. The muscle itself is outside the soft palate. An MRI in the plane of the levator (at 60 degrees to the horizontal) (Fig. 50-3) shows the relationship of the levator and the palatopharyngeus, in close proximity near the midline but diverging as they pass laterally, with the tensor situated lateral to the palate. The sensory supply of the soft palate is predominantly from the lesser palatine nerves, of which several branches pass through the lesser palatine foramina in the palatal process of the sphenoid and through the palatal aponeurosis. The motor supply of the levator, the palatopharyngeus, and the palatoglossus muscles is from the pharyngeal plexus (cranial nerves IX, X, and XI). The musculus uvulae is supplied in normal anatomy by the lesser palatine nerve.25 The tensor veli palatini muscle is supplied by a branch from the trigeminal nerve (V). The aim of surgery should be to restore anatomy as close as possible to normal while minimizing damage to normal anatomic structures.26 Wherever possible, the palate should be closed without lateral releasing incisions. Whether this is possible depends on the type, extent, and width of the cleft. In isolated clefts of the palate, the need for lateral releasing incisions increases with the extent and width of the cleft, but such incisions are required in less than 20% of cases (most often in wide, U-shaped clefts, often associated with Pierre Robin sequence) (Fig. 50-4). Fig. 50-4 The need for lateral releasing incisions in a consecutive series of repairs of isolated cleft palates. Fig. 50-5 A, The “traditional” von Langenbeck incisions. B, Modified incisions. Lateral releasing incisions are likely to be necessary if the cleft at the back of the hard palate is wider than 10 mm (at the age of repair at 6 months). In very wide U-shaped clefts, if the need for lateral releasing incisions is determined early, they are made with subperiosteal elevation of the oral mucoperiosteum both laterally and medially.27,28 Extending the incision into the soft palate behind the alveolus is not necessary (Fig. 50-5). Closure of the hard palate without lateral releasing incisions depends on: • The drawbridge effect—converting the sloping palatal mucoperiosteal flaps to become more horizontal • Unfolding of the flaps, especially if the mucoperiosteum is infolded • Mobilization of the greater palatine neurovascular pedicles, if necessary • Division of the oral component of the tensor palatini insertion, if necessary Unless the cleft is very wide, and lateral releasing incisions are determined to be necessary at the beginning of the procedure, incisions are made at the junction of the oral and nasal mucosa. This junction is usually clearly seen, because the nasal mucosa is more pink (or often more pigmented in darker-skinned individuals) and telangiectatic and is usually on the oral side of the cleft (Fig. 50-6, A). If the residual cleft extends into the hard palate, the oral flap is elevated to the edge of the bony palatal cleft with a Beaver knife with a No. 69 blade. With an appropriate dental scaler or semisharp dissector, the mucoperiosteal flaps are lifted from the hard palate. At this stage the posterior border of the hard palate should be exposed in a subperiosteal plane (Fig. 50-6, B). Dimples and irregularities commonly occur on the oral mucosa at the point where the oral mucous glands are attached deeply to the posterior border of the hard palate (Fig. 50-6, C). By extending the incision backward, using a combination of a dental scaler and knife, the mucous glands are lifted intact (Fig. 50-6, D) to expose the white tendinous nasal component of the tensor veli palatini tendon (Fig. 50-6, E).
Cleft Palate Repair With Minimal Hard Palate Dissection and Radical Muscle Reconstruction
Brian C. Sommerlad
KEY POINTS
BACKGROUND AND HISTORY
RECONSTRUCTIVE PRINCIPLES
Rationale for the Technique
PATIENT SELECTION AND EVALUATION
MANAGEMENT ALGORITHM
Timing of Repair
Preoperative and Perioperative Factors
SURGICAL TECHNIQUE
Instrumentation

Anatomy
Hard Palate
Soft Palate
Technique
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine