Key points
- •
The palate is divided functionally into the hard palate, which provides structural support and is a growth center for the maxilla, and the soft palate, which provides velopharyngeal competence.
- •
The levator vela palatini muscles are the principal motors of the velar component of velopharyngeal closure.
- •
In the cleft palate, the levators are positioned sagittally , running posterior to anterior and inserting onto the posterior edge of the hard palate. This configuration prevents the levator from exerting its upward, backward, and lateral pull.
- •
Cleft palate repair must include complete release of the levator from its abnormal attachments to the posterior edge of the hard palate medially, the tensor aponeurosis, and the superior constrictor laterally.
- •
Outcome measures for cleft palate repair include speech quality and palatal integrity.
Introduction
Human speech is supported by complex anatomic structures and nuanced physiologic processes. A cleft palate is a developmental rent through this system and must be approached in this regard. Palatoplasty is speech surgery. The surgeon addressing a cleft palate must do so with an eye toward repairing the form and function of the dynamic physical structures that work in complex harmony to manipulate air pressure emanating from the respiratory tract into sounds intelligible to others as speech. Herein, the authors begin with a discussion of the anatomy relevant to palatoplasty. Perioperative considerations are then addressed. A broad range of surgical options has evolved over time; these are discussed in their historical context. Next, the authors present a detailed description of their preferred surgical approach. Postoperative care is then described. An examination of recent trends and controversies in the field is then offered. Finally, an approach to outcomes assessment is discussed. It is hoped that this monograph will be of use in guiding others as they embark on the highly challenging, but equally rewarding, task of perfecting the palatoplasty.
Pertinent anatomy
The primary palate includes all structures anterior to the incisive foramen (the premaxilla). The secondary palate comprises the hard palate posterior to the incisive foramen and the soft palate. The muscular soft palate, or velum, is found posterior to the hard palate. Clefts of the secondary palate take the form of a midline bony deficiency resulting in the dissociation of the vomer from the hard palate.
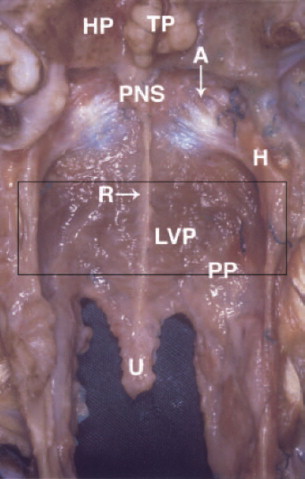
The soft palate may be divided into 3 sections from a functional perspective: the anterior 25%, the middle 50%, and the posterior 25%. In a series of fresh cadaver dissections, Huang and colleagues found that fibers of the levator veli palatine occupy the middle 50% of the soft palate. The levators take their origin from the posteromedial aspect of the junction of the cartilaginous and bony segments of the eustachian tube. The left and right levators insert into one another in the palatal midline, forming a sling suspending the soft palate from the cranial base ( Fig. 1 ). The levator functions as the motor of the velum. Also in the middle 50% of the soft palate, the palatopharyngeus muscle originates with an inferior head on the oral surface of the levator and a superior head on the nasal surface of the levator and runs inferiorly as the posterior tonsillar pillar. Originating from the dorsolateral transverse fibers of the tongue, the palatoglossus travels cephalad as the anterior tonsillar pillar before fanning out to insert in the middle 50% of the soft palate as the most superficial muscle of the velum. The anterior 25% of the soft palate is relatively static. Specifically, the tensor veli palatini originates from the greater wing of the sphenoid and the superolateral aspect of the eustachian tube. It then descends nearly vertically to hook around the anterior aspect of the hamulus and inserts into the fibrous tensor aponeurosis in the anterior 25% of the velum (see Fig. 1 ; Fig. 2 ). The palatopharyngeus, palatoglossus, and muscularis uvulae are found in the posterior 25% of the soft palate. The muscularis uvulae takes its origin at the tensor aponeurosis and courses posteriorly as a paired midline structure to terminate at the base of the uvula.
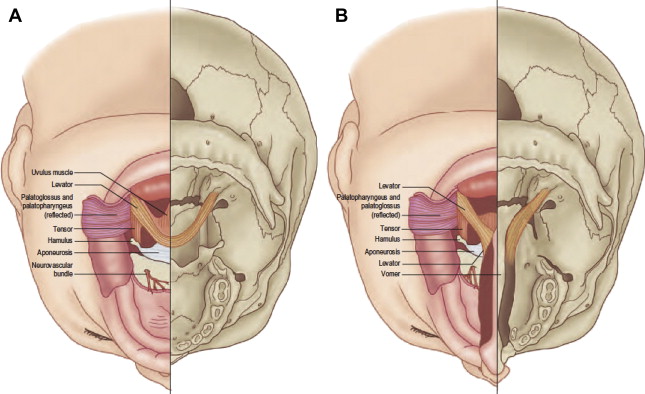
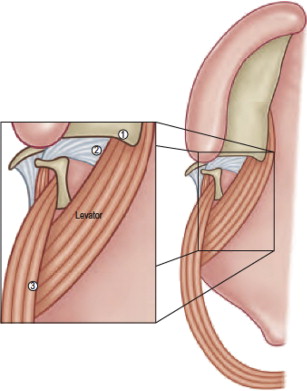
In the normal palate, the levator forms a muscular sling that suspends the soft palate from the cranial base (see Fig. 1 A). Running from its origins at the cranial base to its insertion into its partner in the velum, the levator takes a downward, forward, and medial course that facilitates a cranial, posterior, and lateral pull on the soft palate during velopharyngeal closure. In the normal state, the levators take a transverse course , running horizontally within the middle 50% of the velum, whereas the cleft palate’s levators are positioned sagittally , running posterior to anterior inserting onto the posterior edge of the hard palate. This clefted configuration prevents the levator, the principal motor of the velar component of velopharyngeal closure, from exerting its upward, backward, and lateral pull. Moreover, in the cleft palate, the levator has 3 abnormal associations that must be addressed in repairing the defect: an insertion onto the posterior medial edge of the hard palate, associations with the aponeurosis of the tensor veli palatini, and lateral adhesions to the superior pharyngeal constrictor (see Fig. 1 B; Fig. 3 ).
As the levator and tensor take their origins from the eustachian tube, the effects of clefting on this structure must also be considered. Although there is controversy as to whether the tensor or the levator is more significant in tubal dilation, there is likely a synergistic mechanism. In one suggested configuration, the tensor contracts to exert a force on the lateral eustachian tube, dilating the lumen, while the levator rotates the medial lip of the tubal cartilage to optimize the tensor’s vector. It stands to reason that the altered morphology of the levator and tensor in the cleft palate may impair their function as tubal dilators.
Pertinent anatomy
The primary palate includes all structures anterior to the incisive foramen (the premaxilla). The secondary palate comprises the hard palate posterior to the incisive foramen and the soft palate. The muscular soft palate, or velum, is found posterior to the hard palate. Clefts of the secondary palate take the form of a midline bony deficiency resulting in the dissociation of the vomer from the hard palate.
The soft palate may be divided into 3 sections from a functional perspective: the anterior 25%, the middle 50%, and the posterior 25%. In a series of fresh cadaver dissections, Huang and colleagues found that fibers of the levator veli palatine occupy the middle 50% of the soft palate. The levators take their origin from the posteromedial aspect of the junction of the cartilaginous and bony segments of the eustachian tube. The left and right levators insert into one another in the palatal midline, forming a sling suspending the soft palate from the cranial base ( Fig. 1 ). The levator functions as the motor of the velum. Also in the middle 50% of the soft palate, the palatopharyngeus muscle originates with an inferior head on the oral surface of the levator and a superior head on the nasal surface of the levator and runs inferiorly as the posterior tonsillar pillar. Originating from the dorsolateral transverse fibers of the tongue, the palatoglossus travels cephalad as the anterior tonsillar pillar before fanning out to insert in the middle 50% of the soft palate as the most superficial muscle of the velum. The anterior 25% of the soft palate is relatively static. Specifically, the tensor veli palatini originates from the greater wing of the sphenoid and the superolateral aspect of the eustachian tube. It then descends nearly vertically to hook around the anterior aspect of the hamulus and inserts into the fibrous tensor aponeurosis in the anterior 25% of the velum (see Fig. 1 ; Fig. 2 ). The palatopharyngeus, palatoglossus, and muscularis uvulae are found in the posterior 25% of the soft palate. The muscularis uvulae takes its origin at the tensor aponeurosis and courses posteriorly as a paired midline structure to terminate at the base of the uvula.
In the normal palate, the levator forms a muscular sling that suspends the soft palate from the cranial base (see Fig. 1 A). Running from its origins at the cranial base to its insertion into its partner in the velum, the levator takes a downward, forward, and medial course that facilitates a cranial, posterior, and lateral pull on the soft palate during velopharyngeal closure. In the normal state, the levators take a transverse course , running horizontally within the middle 50% of the velum, whereas the cleft palate’s levators are positioned sagittally , running posterior to anterior inserting onto the posterior edge of the hard palate. This clefted configuration prevents the levator, the principal motor of the velar component of velopharyngeal closure, from exerting its upward, backward, and lateral pull. Moreover, in the cleft palate, the levator has 3 abnormal associations that must be addressed in repairing the defect: an insertion onto the posterior medial edge of the hard palate, associations with the aponeurosis of the tensor veli palatini, and lateral adhesions to the superior pharyngeal constrictor (see Fig. 1 B; Fig. 3 ).
As the levator and tensor take their origins from the eustachian tube, the effects of clefting on this structure must also be considered. Although there is controversy as to whether the tensor or the levator is more significant in tubal dilation, there is likely a synergistic mechanism. In one suggested configuration, the tensor contracts to exert a force on the lateral eustachian tube, dilating the lumen, while the levator rotates the medial lip of the tubal cartilage to optimize the tensor’s vector. It stands to reason that the altered morphology of the levator and tensor in the cleft palate may impair their function as tubal dilators.
Goals of surgery
Velopharyngeal competence that supports normal speech production is sine qua non for success in palatoplasty. Velar anatomy must also be restored to maximize eustachian tube function and support hearing, thus minimizing the risk for the development of recurrent otitis media secondary to insufficient tubal dilation and impaired drainage. Nasal air emission and subsequent hypernasality and speech distortion must be obfuscated by a watertight barrier between the oral and nasal cavities. Separating the oral cavity from the nasal cavity will also prevent the nasal regurgitation of fluid and food. A universal requirement essential to all these goals is a tension-free watertight repair of the palate to minimize subsequent scarring and fistula formation ( Fig. 4 ).
Patient assessment and perioperative considerations
Timing of the Repair
The palate is divided functionally into the hard palate (serving as structural support and a growth center for the maxilla) and the soft palate (providing velopharyngeal competence). Because maxillary growth and speech development do not occur in unison, there is disagreement as to the timing of palatoplasty that is most compatible with normal speech development without harming midface growth. Some fear that a soft palate cleft persisting past 1 year of age may impair speech development and, therefore, favor early palatoplasty. Those concerned that early palatoplasty may impair midface growth argue for delaying intervention until midface growth is nearing completion. Some address this discrepancy by temporally separating soft palate repair from hard palate repair to uncouple the perceived deleterious effects of a late soft palate repair (impaired speech development) from those of an early hard palate repair (stunted maxillary growth).
The literature on this controversy is difficult to parse because of the variability in surgical timing (3 months to 2 years of age for velum and 6 months to adolescence for hard palate) and technique. Rohrich and colleagues detected a statistically significant speech deficiency with delayed (48.6 months) versus early (10.8 months) hard palate closure and no improvements in maxillofacial growth with later repair. In a series of 2000 patients, Koberg and Koblin observed that palatoplasty between 8 and 15 years of age caused the greatest degree of maxillary growth disturbance and argued that hard palate repair should be delayed until after 15 years of age. Alternatively, Robertson and Jolleys saw no difference in occlusion or facial profile between patients undergoing palatoplasty from 12 to 15 months of age and those undergoing palatoplasty at 5 years of age. The authors hold that the presently available evidence of impaired midface growth secondary to early palatoplasty is not sufficiently convincing to justify sacrificing the opportunity to correct soft palate anatomy and facilitate normal speech development with early palatoplasty. These data are also not so robust as to rationalize the additional morbidity and cost associated with a 2-stage repair protocol. It is the authors’ standard practice to repair palatal clefts in a single-stage procedure at approximately 1 year of age.
Feeding
Palatal clefts directly affect normal feeding mechanisms: the connection between the oral and nasal cavities permits nasal regurgitation of fluid and food, and swallowing may potentially be affected by velopharyngeal incompetence (VPI). Swallowing difficulties may be addressed by positioning the infant at 45° to 60° from horizontal to exploit gravity during feeding. The clefted velum renders the creation of an intraoral vacuum impossible. A cleft lip in addition to cleft palate yields difficulties in forming a labial seal around the nipple and impairs sucking.
Feedings should be delivered to the posterior portion of the tongue to minimize the infant’s dependence on achieving a vacuum. Specialized bottles (Pigeon [Philips Healthcare, Andover, MA] and Haberman feeders [Medela, Inc, McHenry, IL]) are marketed and are designed to allow the caregiver to actively dispense the liquid. Ideally, the infant is weaned entirely from the bottle and drinking from a sippy cup before palatal repair.
Airway Compromise and Pierre Robin Sequence
Patients with cleft palates may preoperatively have airway compromise caused by associated multilevel airway disease. Postoperatively, alterations in airway anatomy secondary to manipulation of the velopharynx or swelling (in the immediate postoperative period) may also result in airway compromise. A thorough evaluation for airway compromise, which may be heralded by episodes of desaturation during feeding or sleep, is mandatory. Should evidence of airway compromise be detected, a complete multilevel examination in conjunction with an otolaryngologist is necessary. The airway in children with Pierre Robin sequence (PRS) is of particular concern. PRS is a constellation of physical findings including posterior displacement of the tongue (glossoptosis), a receding mandible (retrognathia), and resulting compromise of the airway. The U-shaped palatal clefts frequently seen with this condition are thought to result from the retropositioned mandible and posteriorly displaced tongue interfering with the fusion of the palatal shelves (Editor note: PRS is discussed in the article “Surgical Considerations in Pierre Robin Sequence” elsewhere in this issue by Justine Lee and James P. Bradley).
Current practice and its origins
Repair of the Hard Palate
Hard palate repair can be divided into techniques that use bipedicled and/or unipedicled flaps. Bipedicled flaps are based on the incisive foramen pedicle anteriorly and the greater palatine pedicle posteriorly. The von Langenbeck repair is a popular technique that incorporates bipedicled flaps. In unipedicled flaps, the anterior pedicle is divided and the palatal flaps are based exclusively on the greater palatine pedicle. The Veau–Wardill–Kilner repair (VWK or VY push-back) and the 2-flap palatoplasty are common examples of a unipedicled repair.
Von Langenbeck described his bipedicled repair in the nineteenth century. Adopting Dieffenbach’s earlier introduction of the lateral relaxing incision, this repair raises bilateral bipedicled mucoperiosteal flaps. The lateral border of these flaps is an incision along the attached gingiva that runs posteriorly to a point lateral to the hamulus, approximately 1 cm posterior to the maxillary tuberosity. A mucosal incision along the border of the cleft, between the oral and nasal mucosa, marks the flap’s medial extent. Nasal mucosa flaps are sutured to one another in the midline to repair the nasal lining defect (often incorporating a vomer flap). The bipedicled hard palate flaps are advanced to close the oral side of the defect.
The VWK repair and the 2-flap palatoplasty are based on bilateral unipedicled flaps for hard palate reconstruction. The VWK repair took its origins from Veau’s VY advancement flap series of 1922. Although conceptually similar to the von Langenbeck repair described earlier, the anterior pedicle is divided to yield unipedicled flaps, and the mucoperiosteal flaps are approximated with the incorporation of an anteriorly based VY advancement flap. Some individuals hold that this repair lengthens the soft palate as the mucoperiosteal flaps are advanced posteriorly and may, therefore, improve velopharyngeal competence. Others express concern that the degree of hard palate periosteal dissection that is necessary may impair midface growth. The authors of this work are unsure of the degree to which hard palate push back contributes to velar length or function. In the 2-flap palatoplasty (also a unipedicled flap technique), flaps similar to those of the VWK repair are raised but extend anteriorly to incorporate the alveolar mucosa when involved.
Repair of the Soft Palate
Although the hard palate is a static structure, the soft palate rapidly changes its configuration to determine the aperture of the velopharynx, thus mediating speech production. Von Graefe and Roux first approached velar repair in the early nineteenth century, focusing their efforts on approximating the 2 sides of the defect. Although these researchers addressed the velum’s aberrant morphology, Veau, Wardill, and Kilner endeavored to improve velar dynamics with their push back or straight-line procedures designed to lengthen the soft palate with repair of the hard palate in an effort to better position the velum to participate in velopharyngeal function. The anatomic basis for cleft velar dynamics was first directly addressed in 1969 by Kriens, with his intravelar veloplasty (IVVP). The IVVP reoriented the clefted velar levators from their pathologic sagittal course to their physiologic horizontal course, repairing the levator sling. Furlow described his “double-opposing Z-plasty” in 1986. This imaginative soft palate repair uses paired Z-plasty flaps to simultaneously repair the levator sling and lengthen the soft palate. The effectiveness of the IVVP incorporated into the Furlow repair stems from the fact that the levator is transferred within a vascularized mucosal-muscular flap, eliminating the need to completely dissect the levator free from both the nasal and oral mucosae. In transferring the abnormal levators from a sagittal to horizontal configuration, they are overlapped and placed on functional tension to reconstruct the levator sling. Because Z-plasties typically lengthen in one direction at the expense of shortening tissue perpendicularly, by lengthening the velum via a Z-plasty, the Furlow palatoplasty narrows the caliber of the velopharyngeal port. The double-opposing Z-plasty, thus, simultaneously serves as a palatoplasty and a pharyngoplasty.
Two-Stage Palatoplasty
Because of the controversy regarding the timing of palatoplasty discussed earlier, certain researchers prefer to separate hard and soft palate repair into 2 phases. This practice is well described by Rohrich and Gosman, who advocate a 2-stage repair whereby both stages are performed fairly early. In brief, Rohrich and Gosman’s protocol consists of cleft lip and soft palate repair at 3 to 6 months, with hard palate repair following at 15 to 18 months. It is posited that isolated repair of the lip and velum before hard palate repair molds the anterior and posterior alveolar arch segments, respectively. This molding is thought to yield a narrowed hard palate cleft that allows a tension-free repair with minimized mucoperiosteal elevation (and its attendant adverse growth effects) at the second stage operation.
The authors’ approach: Furlow palatoplasty
Soft Palate
Markings
The double-opposing Z-plasties are comprised of 2 oral flaps and 2 nasal flaps. These flaps include 2 anteriorly based mucosal flaps and 2 posteriorly based musculomucosal flaps. The posteriorly based oral musculomucosal flap is designed on the patients’ left side by convention. The velar relaxing incisions ( Fig. 5 ) are drawn in the crease at the junction of the vertical cheek sidewalls and the horizontal velar shelves. The relaxing incisions extend posteriorly from the maxillary tuberosity to the region of the mandibular retromolar trigone. Anteriorly, they extend onto the hard palate along the attached gingiva. Then, marks are placed on the hamuli, uvular bases, and junctions of the hard and soft palates bilaterally. The medial cleft margin incision is marked. This incision is made slightly on the oral side of the cleft margin in an effort to cheat extra tissue for the nasal lining repair. The medial uvular surfaces are marked to be demucosalized. The lateral limb incision of the left-sided posteriorly based oral musculomucosal flap is designed by joining the marked left hamulus laterally to the junction of the hard and soft palates medially, creating an approximately 60° flap. The lateral limb incision of the right-sided anteriorly based oral mucosal flap is designed by joining the right-sided uvular base medially to the right-sided marked hamulus laterally, creating a flap between 60° and 90°. A mucosal bridge must be preserved between the relaxing incisions and the lateral extent of the lateral limb incisions.
Incisions and flap elevation
The medial uvular halves are demucosalized ( Fig. 6 ) and tagged with a suture in each distal tip. The left-sided cleft-margin incision and the lateral limb incision of the left-sided posteriorly based oral musculomucosal flap ( Fig. 7 ) are made. Dissection begins near the junction of the hard and soft palates on the left side; the levator is identified medially at its insertion into the posterior edge of the hard palate. This connection is severed, and dissection continues laterally ( Fig. 8 ). The tensor aponeurosis is identified at the posterior edge of the hard palate with its abnormal attachment to the levator. The aponeurosis is incised. Lateral dissection releases the levator from its abnormal associations with the superior constrictor ( Fig. 9 ). The tip of the left-sided, posteriorly based oral musculomucosal flap is tagged with a traction stitch. Dissection proceeds posteriorly, between the left-sided levator and the nasal mucosa, until the junction of the uvula and velum is reached, leaving submucosa with the nasal lining. The levator is bluntly swept free from any remaining association with the superior constrictor ( Figs. 10 and 11 ) and radically retroposed to its anatomic transverse orientation ( Fig. 12 ). The levator and the superior constrictor are now at nearly 90° to one another (see Fig. 11 B). Again, the levator must be completely released from its abnormal attachments to the posterior edge of the hard palate medially, the tensor aponeurosis, and the superior constrictor laterally, as achieved in this dissection (see Figs. 3 and 12 ).






