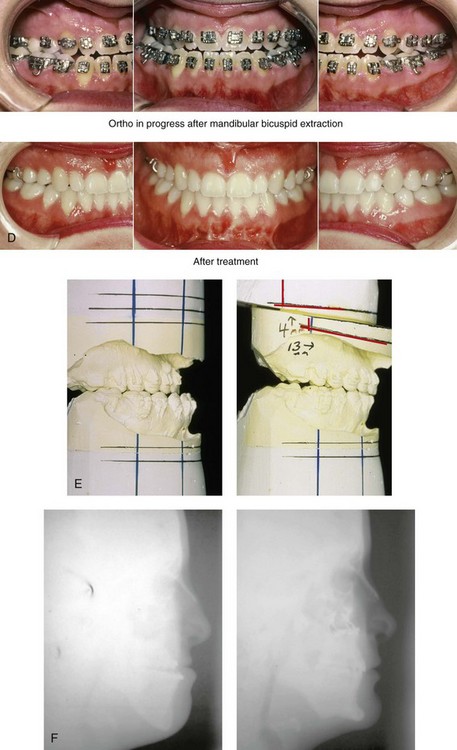
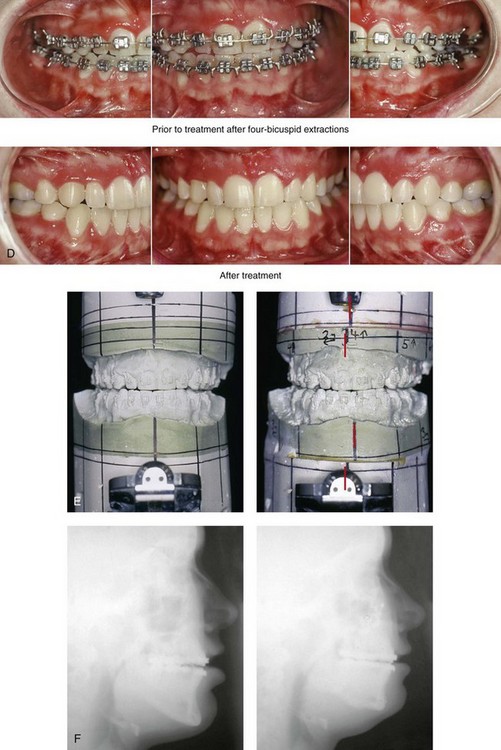
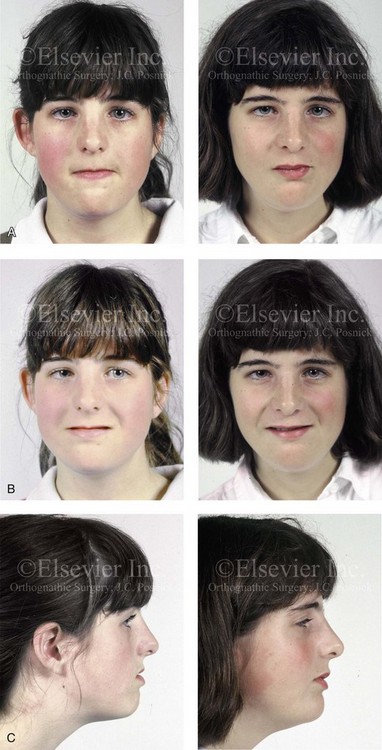
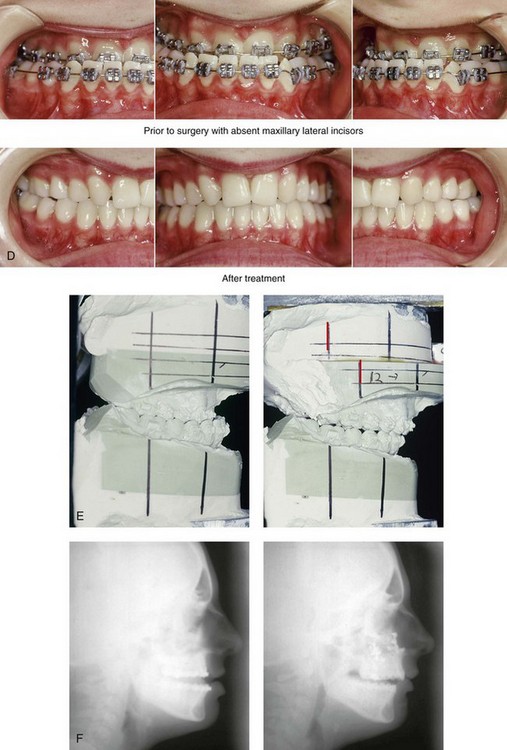
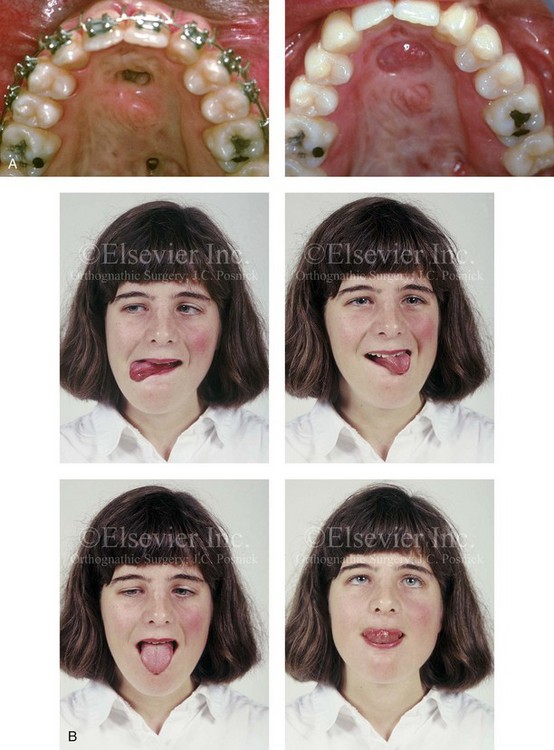
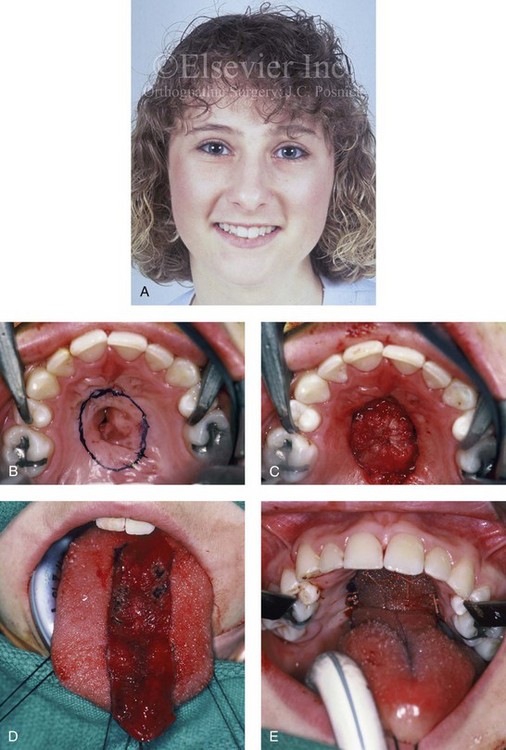
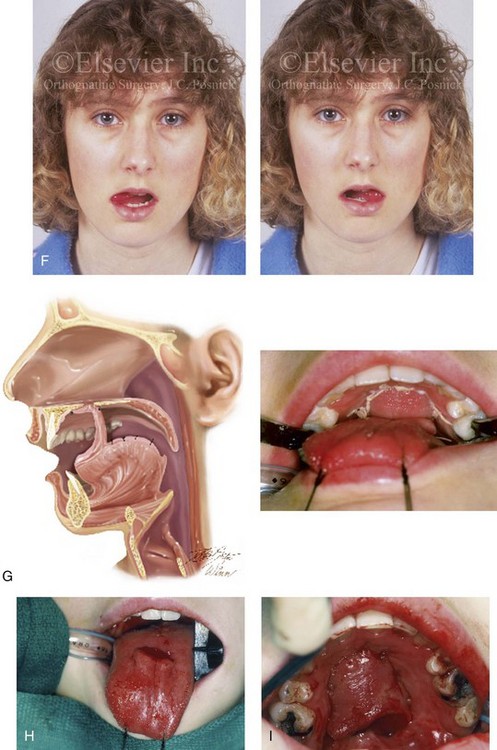
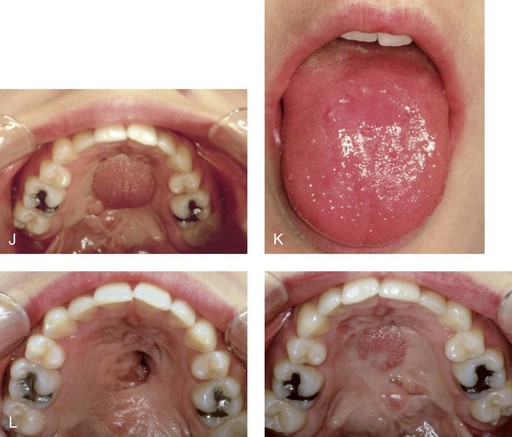
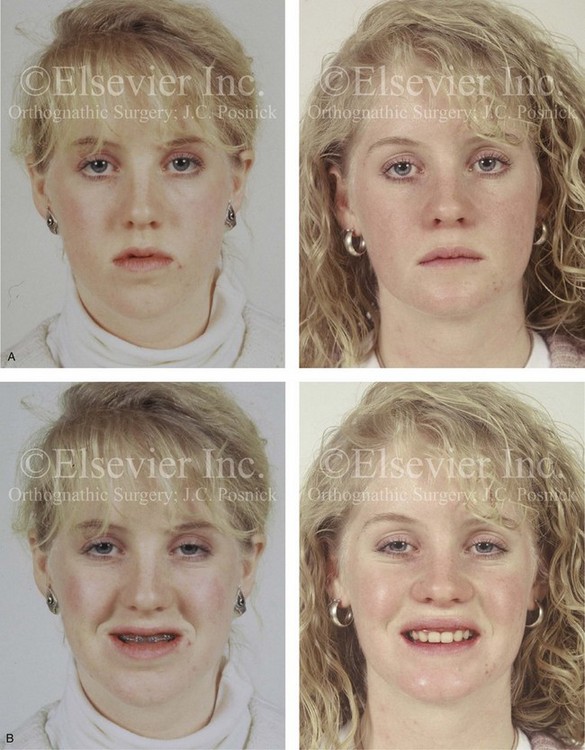
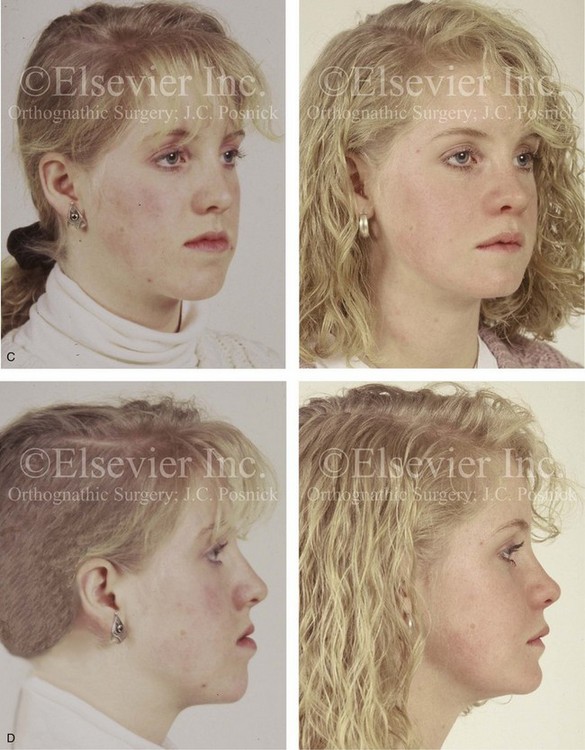
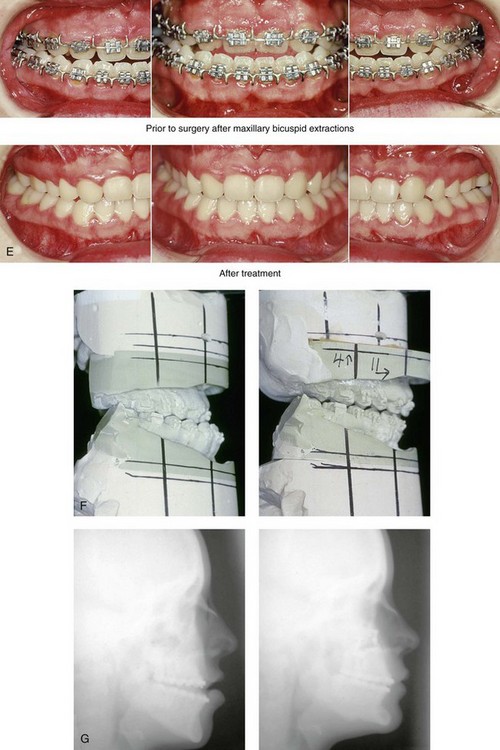
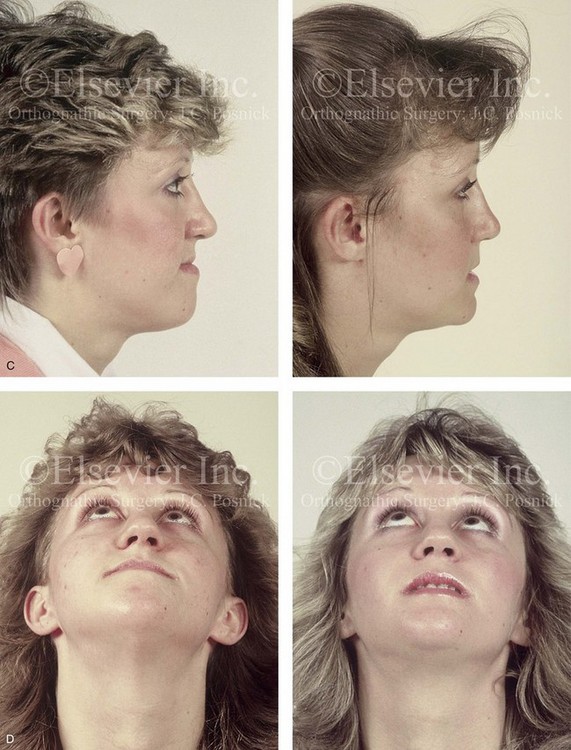
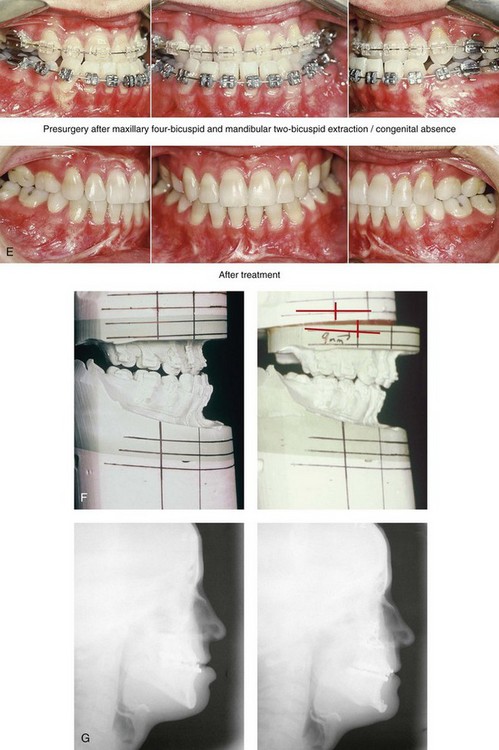
34 • Facial Growth Implications of Cleft Palate Repair in the Infant with Isolated Cleft Palate • Timing of Orthognathic Surgery • Residual Deformities in the Adolescent with Isolated Cleft Palate • Orthodontic Considerations in the Patient with Isolated Cleft Palate with a Jaw Deformity • Immediate Presurgical Assessment • Orthognathic Surgical Approach for Isolated Cleft Palate • Clinical Management after Initial Surgical Healing • Orthognathic Surgery for Isolated Cleft Palate: Review of Study • Controversies and Unresolved Issues Ross documented that at least 20% of Caucasian individuals with ICP who undergo repair during infancy will experience maxillary hypoplasia that results in malocclusion that is not responsive to either traditional or compensatory orthodontic maneuvers alone.86 Chen and colleagues reported on horizontal maxillary growth in both children and adults with Eastern Chinese ethnic backgrounds and with unoperated and operated ICP.14 There were two study groups: individuals in Group 1 had non-syndromal and unoperated ICP that was evaluated during the mixed dentition (n = 16); individuals in Group 2 had non-syndromal and unoperated ICP that was evaluated during the permanent dentition (n = 25). The control groups included patients with ICP who underwent repair during childhood as well as non-cleft individuals with Class I occlusion that was evaluated during both the mixed and permanent dentitions. Lateral cephalograms of all subjects were analyzed. The results of the mixed dentition groups showed almost normal sagittal growth in unoperated patients except for the reduced anterior-posterior maxilla length. In contrast, the operated patients showed reduced length of both the maxilla and mandible, as well as a clockwise rotation of the mandible. The analysis of the permanent dentition groups showed that in both the unoperated and operated ICP patients, there were reductions in maxilla length, mandibular protrusion, and maxillary retrusion. Interestingly, there appeared to be no correlation between maxillary growth restriction and the extent of the congenital clefting of the secondary palate (i.e., soft palate only versus hard and soft palate). The authors concluded that, for individuals born with ICP, the etiology of the maxillomandibular deficiency likely results from a combination of factors, including the intrinsic primary (cleft) defect; secondary hypoplasia as a result of the surgical repair during infancy (iatrogenic); and functional (environmental) factors (e.g., the effects of muscles of mastication, respiratory patterns, mandibular rest posture; see Chapter 4). These results were similar to those of Yoshida and colleagues, who found that individuals with ICP frequently end up with maxillary horizontal deficiency and clockwise rotation of the maxillomandibular complex that tend to become worse as the child reaches adulthood.99 A significant percentage of adolescent patients who were born with ICP will present with a jaw deformity that requires, at minimum, a maxillary Le Fort I (down-fracture) osteotomy to align the jaws.5,85 When indicated, this is combined with mandibular and chin osteotomies to achieve improved facial proportions and with intranasal procedures (i.e., septoplasty and inferior turbinate reduction) to improve nasal breathing. The facial reconstructive and dental rehabilitation of an individual with ICP is best delivered via collaborative care provided by appropriate medical and dental specialists.6,62,71 It is no longer justified for individual practitioners—whether they are surgeons, orthodontists, restorative dentists, speech pathologists, or otolaryngologists—to carry out extensive treatment without informing the patient and his or her family of available options and considering clinical input from the other specialists who are caring for the patient. The primary cleft surgeon completes the patient’s palate repair during infancy, and this is followed by pharyngeal procedures later during the patient’s childhood if they are required to improve velopharyngeal function. The surgeon is also likely to play an important role in directing the patient’s care throughout adolescence and into adulthood. If the cleft surgeon is not trained in skeletal procedures, then a timely and seamless transition to the maxillofacial surgeon who will continue on with the patient’s reconstruction is necessary. The orthodontist identifies early abnormal facial growth patterns and may carry out interceptive treatment.6,10,11,18,19,27,34,51,55,64,65,87,90,91 Definitive orthodontic treatment is coordinated with orthognathic surgery, when indicated.33 Extensive compensatory orthodontic treatment is likely to jeopardize periodontal health and to lead to dental relapse with recurrent malocclusion. Camouflage orthodontics should be avoided for these reasons and only be entered into with full disclosure to the family and other treating clinicians. Before orthognathic surgery is performed, the speech pathologist performs an evaluation to assess the patient’s velopharyngeal function; this will ideally include nasoendoscopic instrumentation. Such evaluation is important, because velopharyngeal function may deteriorate after maxillary Le Fort I osteotomy with advancement (see Chapter 8). Velopharyngeal closure that was adequate before surgery may become borderline afterward, and closure that was borderline may become inadequate. In the past, investigators have speculated that, if the distraction (DO) technique is used to advance the Le Fort I osteotomy, then velopharyngeal function will not deteriorate. However, clinical studies have now documented that velopharyngeal function will deteriorate in a similar fashion after Le Fort I advancement when either DO or standard techniques are used.12,13,35,37,50,54,58,61,72,89,94 Articulatory distortions that result from the jaw discrepancy and malocclusion also are identified by the speech pathologist, and cause-and-effect relationships are determined. It is known that the successful orthodontic and surgical correction of crossbites, open bite, residual palatal fistulas, and negative overjet will generally correct the presenting articulation errors (see Chapter 8). The otolaryngologist plays a role in the assessment of upper airway and middle ear function. Chronic nasal obstruction and sinusitis are frequent in the patient with a cleft palate. Mucous trapping may also be a problem after a pharyngeal flap procedure. If sleep apnea is suspected, an attended polysomnogram should be carried out (see Chapter 26). If intranasal procedures (i.e., septoplasty and inferior turbinate reduction) are needed to improve breathing, they should be simultaneously carried out in conjunction with orthognathic surgery (see Chapter 10). The correction of the jaw deformity associated with ICP is best carried out when the skeleton is mature and before the patient completes high school, if feasible. Maxillofacial growth is generally complete between the ages of 14 and 16 years in girls and between the ages of 16 and 18 years in boys. However, skeletal growth is variable, and it may be further clarified via the analysis of sequential cephalometric radiographs (see Chapter 17). Input from the patient and the family regarding the timing of surgery and the patient’s functional needs (e.g., breathing, speech, chewing, swallowing, body image, self-esteem) are also important considerations. As early as 1986, clinicians clarified through preliminary studies that, if jaw surgery is undertaken in the growing patient with a cleft palate patient, revision orthognathic surgery will likely be required after skeletal maturity is reached.95–98 More recently, other investigators have tested this theory by proceeding with Le Fort I osteotomy involving DO methods during the mixed dentition. Studies to date indicate that a Le Fort I osteotomy carried out during the mixed dentition, whether with a standard or a DO technique, results in limited or no further horizontal maxillary growth.17,36,46,73,74 As the mandible continues to grow, an Angle Class III malocclusion recurs with the need for either additional Le Fort I advancement or mandibular set-back. The adolescent or adult patient with ICP who is referred for orthognathic evaluation will have an intact alveolar ridge and generally will have a full complement of teeth. However, these individuals may present with one or more of the following residual cleft-related problems (Figs. 34-1 through 34-9): Figure 34-1 A 19-year-old woman who was born with isolated cleft palate. The maxillary deformity is characterized primarily by horizontal deficiency. The patient underwent mandibular first bicuspid extractions. She was referred to this surgeon and agreed to a comprehensive orthodontic and orthognathic surgical approach. The patient’s procedures included Le Fort I osteotomy (horizontal advancement, vertical lengthening, and clockwise rotation) with interpositional grafting; osseous genioplasty (vertical reduction and horizontal advancement); and septoplasty and inferior turbinate reduction. A, Frontal views in repose before and after reconstruction. B, Frontal views with smile before and after reconstruction. C, Profile views before and after reconstruction. D, Occlusal views during orthodontics and after reconstruction. E, Articulated dental casts indicate analytic model planning. F, Lateral cephalometric radiographs before and after reconstruction. A, C, D (top center and bottom center), E (right), from Posnick JC: Skeletal stability and relapse patterns after Le Fort I osteotomy using miniplate fixation in patients with isolated cleft palate. Plast Reconstr Surg 94:51, 1994. Figure 34-2 A 19-year-old woman who was born with isolated cleft palate. The deformity is characterized by vertical maxillary excess and jaw asymmetry. The patient underwent four-bicuspid extractions. She was referred to this surgeon and agreed to a comprehensive orthodontic and orthognathic approach. The patient’s procedures included Le Fort I osteotomy (minimal horizontal advancement, clockwise rotation, vertical intrusion, and asymmetry correction); bilateral sagittal split ramus osteotomies (correction of asymmetry); osseous genioplasty (vertical reduction); and septoplasty, inferior turbinate reduction, and nasal recontouring. A, Frontal views in repose before and after reconstruction. B, Frontal views with smile before and after reconstruction. C, Profile views before and after reconstruction. D, Occlusal views with orthodontics in progress and after reconstruction. E, Articulated dental casts indicate analytic model planning. F, Lateral cephalometric radiographs before and after reconstruction. Figure 34-3 A 17-year-old girl who was born with isolated cleft palate. The deformity is characterized primarily by horizontal maxillary deficiency and a palate fistula. The patient was referred to this surgeon and agreed to a comprehensive orthodontic and orthognathic approach. The maxillary lateral incisors were congenitally absent. The patient’s procedures included a Le Fort I osteotomy (horizontal advancement and vertical lengthening) with interpositional grafting. One year after the initial procedure, she underwent an anterior-based dorsal tongue flap procedure for palatal fistula closure. A, Frontal views in repose before and after reconstruction. B, Frontal views with smile before and after reconstruction. C, Profile views before and after reconstruction. D, Occlusal views with orthodontics in progress and after reconstruction. E, Articulated dental casts indicate analytic model planning. F, Lateral cephalometric radiographs before and after reconstruction. A, C, D, F, from Posnick JC, Tompson B: Cleft–orthognathic surgery: complications and long-term results. Plast Reconstr Surg 96:255, 1995. Figure 34-4 The patient from Figure 34-3 is shown after the successful placement of an anterior-based dorsal tongue flap for palatal fistula closure. A, Palatal views before and after the tongue-flap closure of a recalcitrant fistula. B, Facial views of the patient demonstrating a full range of tongue motion after the harvesting of tissue for palatal reconstruction. Figure 34-5 A 17-year-old girl with a recalcitrant fistula at the incisal foramen region. The fistula had been present since the time of her initial cleft palate repair, despite several attempts at closure at another institution during the patient’s childhood. She was referred to this surgeon for management. The fistula at the incisive foramen was successfully closed with an anteriorly based dorsal tongue flap. A, Facial views before fistula closure. B, Intraoperative view of the palatal fistula, with ink used to mark the extent of the bony defect. C, Local palatal flaps were developed and turned over for nasal-side closure. D, The elevated anteriorly based dorsal tongue flap is shown. It measured two thirds of the width of the tongue and was approximately 5 cm in length. E, The flap is inset to cover the oral side of the palatal defect. The tongue flap is then sutured to the adjacent palatal tissue three quarters of the way around. The posterior aspect of the flap is not sutured, because this would compromise flap circulation. The oro-tracheal tube can be seen on the side of the tongue. F, Range of motion of the tongue is demonstrated at 10 days after flap inset and before flap release. G, Illustration of a cross-sectional sagittal view of face. The tongue flap is shown inset into the palate. Intra-operative view just 10 days after the procedure is also shown. She is returned to the operating room for flap release and inset. H, Intraoperative view of the dorsum of the tongue just after sectioning of the flap and before recontouring. I, Palatal view of bulky tongue tissue on the roof of the mouth before recontouring. J, Palatal view 3 months after flap inset and before debulking. K, Dorsum of the tongue 3 months after flap inset. L, Palatal views before and 8 months after the tongue flap was placed and debulking procedure completed. M, Demonstration of the range of tongue motion 3 months after flap release. Figure 34-6 A 16-year-old girl who was born with isolated cleft palate. The deformity is characterized by horizontal and vertical deficiency of the maxilla and obstructed nasal breathing. The patient agreed to a comprehensive orthodontic and orthognathic surgical approach. Her maxillary first bicuspids were removed. The patient’s procedures included Le Fort I osteotomy (horizontal advancement and vertical lengthening) with interpositional grafting; osseous genioplasty (vertical reduction and horizontal advancement); and septoplasty and inferior turbinate reduction. A, Frontal views in repose before and after reconstruction. B, Frontal views with smile before and after reconstruction. C, Oblique facial views before and after reconstruction. D, Profile views before and after reconstruction. E, Occlusal views with orthodontics in progress and after reconstruction. F, Articulated dental casts that indicate analytic model planning. G, Lateral cephalometric radiographs before and after reconstruction. Figure 34-7 A woman in her early 20s who was born with isolated cleft palate. The deformity is characterized primarily by the horizontal and vertical deficiency of the maxilla. She was referred to this surgeon and agreed to a comprehensive orthodontic and orthognathic surgical approach. She had a congenital absence of some of her teeth, and also required extractions. All total four bicuspids in the maxilla and two bicuspids in the mandible are missing. The patient’s procedures included Le Fort I osteotomy (horizontal advancement and vertical lengthening) with interpositional grafting; osseous genioplasty (vertical reduction and horizontal advancement); and septoplasty and inferior turbinate reduction. A, Frontal views in repose before and after reconstruction. B, Frontal views with smile before and after reconstruction. C, Profile views before and after reconstruction. D, Worm’s-eye views before and after reconstruction. E, Occlusal views with orthodontics in progress and after reconstruction. F,
Cleft–Orthognathic Surgery
The Isolated Cleft Palate Deformity
Facial Growth Implications of Cleft Palate Repair in the Infant with Isolated Cleft Palate
Coordinated Team Approach
Treatment Protocol
Timing of Orthognathic Surgery
Residual Deformities in the Adolescent with Isolated Cleft Palate




Related posts:
![]() Temporomandibular Disorders: Effects of Occlusion, Orthodontic Treatment, and Orthognathic Surgery
Temporomandibular Disorders: Effects of Occlusion, Orthodontic Treatment, and Orthognathic Surgery
 Short Face Growth Patterns: Maxillomandibular Deficiency
Short Face Growth Patterns: Maxillomandibular Deficiency
![]() Long Face Growth Patterns: Maxillary Vertical Excess with Mandibular Deformity
Long Face Growth Patterns: Maxillary Vertical Excess with Mandibular Deformity
![]() Primary Mandibular Deficiency Growth Patterns with or without Maxillary Arch Constriction
Primary Mandibular Deficiency Growth Patterns with or without Maxillary Arch Constriction
 Maxillary Deficiency with Relative Mandibular Excess Growth Patterns
Maxillary Deficiency with Relative Mandibular Excess Growth Patterns
 Syndromes with Craniosynostosis: Evaluation and Treatment
Syndromes with Craniosynostosis: Evaluation and Treatment
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Cleft–Orthognathic Surgery: The Isolated Cleft Palate Deformity
