CHAPTER 28 Circumvertical Breast Reduction and Mastopexy

Key Points
Summary
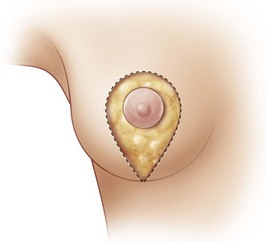
The concept of the circumvertical technique on the skin is to prolong the periareolar technique and shorten the vertical component (Fig. 28.1). At the end of the procedure, the excess skin is distributed in two directions – around the areola and in the vertical component. The skin is adjusted to create an even distribution of wrinkles in both the areola and vertically. The vertical scar does not cross the inframammary fold.
After the vertical reduction from Lassus1,2 and Lejour3,4 other techniques have evolved1,5–7 such as the vertical with the medial pedicle, published by Hall-Findlay8 and the circumvertical one published in 1997, which will be described now.
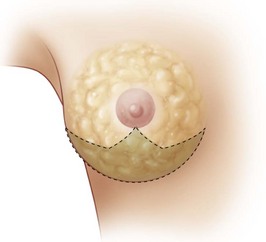
In breast reductions, the differences between the circumvertical and the other vertical techniques lie not only regarding the way the skin is redistributed during the final suture, but also for more profound reasons. These are the W-pattern parenchyma removal (Fig. 28.2), the different ways to build a round-conic projected breast and the absence of a pedicle for the areola transposition. At the end of the surgery the following are observed: a well-shaped breast, with a harmonic distribution of the wrinkles around the areola and the vertical scar never crossing the inframammary fold (IMF).
Operative Technique
Markings
Breast reductions
First, the IMF is marked. The vertical lines passing through the nipple go to the external notch if the areola is to be moved superomedially but they go to the midclavicular line if the areola is only to be moved superiorly. Then the areola is moved into position so that all of the final areolar projection will be above the future submammary fold. The superior border of the areola is then marked on the vertical meridian line. According to the amount of periareolar skin resection needed, 5–6 cm on each side of the nipple are marked, but this could be 4–7 cm if a lateralized areola is to move medially. Then, from the superior mark, a semicircumference is marked and from there two vertical lines are dropped downwards, which converge 2–4 cm above the IMF. The same markings are made on the contralateral side with appropriate adjustments if the breast is larger, smaller, or more ptotic (Fig. 28.3).

Once the whole periareolar skin is de-epithelialized, the skin is undermined at the inferior half of the breast both medially and laterally leaving 1 cm thick subcutaneous tissue to preserve its blood supply (Fig. 28.4A). The inferior half of the breast is also detached from the pectoralis major muscle up to the fourth intercostal space, where the perforator of the fourth intercostal nerve usually emerges (Fig. 28.4B). This way, the dissected breast emerges and holding up the breast with a hook, a Wise pattern resection is marked, which is at the inferior quadrant and at the inferior part of the medial and lateral quadrants (Fig. 28.4C–E). After the resection, the lateral and medial glandular edges are sutured medially in two to three layers using a 3-0 Vicryl suture. If the breast is to project more centrally, both pillars can be imbricated (Fig. 28.4F, G). To have a more projected breast, two to three stitches are placed at the base of the cone in order to keep the pillars together (Fig. 28.4H, I). Once a conic-shaped breast has been obtained, the inferior edge of the parenchyma is fixed to the pectoralis fascia where it now sits using five to seven 3-0 Vicryl separate stitches placed all along what will be the future IMF. At this time, some defatting can be done to give a more even round breast shape. Then the areola is moved to the superior border of the skin and fixed with two to three subdermal 3-0 Vicryl sutures. To finish the surgery, a stitch is placed at 8–10 cm from the inferior part of the skin angle, thus dividing the wound into two parts: the superior round periareolar and the inferior vertical ellipse (Fig. 28.4J). The areola is moved upwards and sutured to the superior skin edge (Fig. 28.4K). The inferior wound is sutured in a vertical fashion with a 3-0 Vicryl subdermal running suture. The periareolar skin is sutured to the areolar border with another a subdermal cinching running suture. This running suture takes big 10–12 mm horizontal bites at the skin dermis and 2–3 mm vertical bites at the areola dermis. This way, after three passes the thread is pulled tight and the skin gathers toward the areola. The suturing is continued all around the areola to give an even distribution of wrinkles all along the areola border and to ensure no dead spaces are left. To finish the surgery, all the wounds are closed with intradermal 5-0 Vicryl suture. Aspiration drains are placed laterally and adhesive tape fixes the wounds. Figures 28.4L, M show the final result. Figure 28.5 shows a representative example.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


