Tan AW, Lim KS, Chong WS. Photoderm Photoimmunol Photomed 2011; 27: 172–5. Three of 26 Singaporean patients with CAD were positive for HIV.
Chronic actinic dermatitis
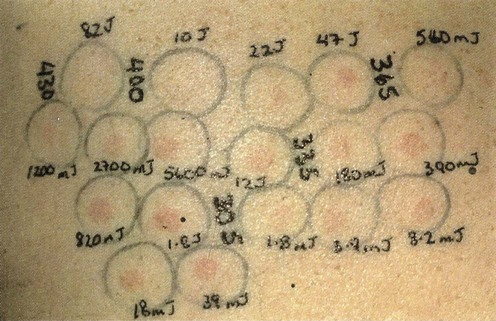
Specific investigations
Chronic actinic dermatitis in Asian skin: a Singaporean experience.
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree






