Cheek Rotation Skin (Imre) Flap to The Lower Eyelid
G. S. PAP
EDITORIAL COMMENT
The McGregor flap (Chapter 12) should be considered as a first option for lower lid reconstruction, because it is simpler to execute, includes potions of the lateral orbicularis muscle, scar is more acceptable and often avoids scleral show.
During the years before World War I, Professor Imre designed the cheek-skin flap that now bears his name (1, 2, 3, 4, 5, 6, 7). The area of the Imre flap can be extended to embrace all tissue from the lower lid downward and from the nasolabial crease laterally (4). This flap uses local tissue similar in texture to that of the defect site, and it avoids a secondary defect. Incisions are placed along the natural wrinkle lines, and repair of a simple or composite defect can be achieved in one operation.
INDICATIONS
The Imre skin flap is indicated for reconstruction of partial or total defects of the lower lid, defects below the lower lid, defects at or below the medial canthus, cicatricial ectropion, and avulsion of the lower lid at the medial canthus. It also can be used, in conjunction with other local skin flaps, for repair of defects in the periorbital region. These include defects at or above the medial canthus, where the Imre flap is used in conjunction with a sliding flap of skin from the forehead at the medial end of the brow; defects at or below the medial canthus, where the Imre flap is used with the adjacent nasal skin as an advancement flap along the nasolabial fold; for correction of an uneven palpebral fissure; or for repositioning of the medial canthal ligament in trauma patients (8).
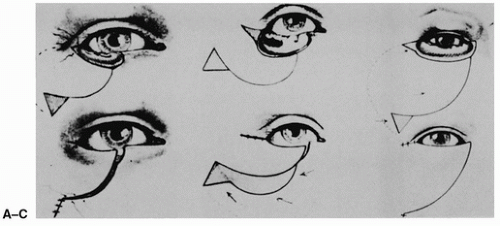 FIGURE 14.1 Imre flap design for various defects of the lower lid. A: For repair of one-third of the lower lid. B: For repair of two-thirds of the lower lid. C: For repair of total loss of the lower eyelid. (From Pap, ref. 8, with permission.)
Related posts: Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
 Wraparound Cartilage Flap for Correction of Cleft-Lip Nasal Deformity Wraparound Cartilage Flap for Correction of Cleft-Lip Nasal Deformity
 Oral Mucosal Flaps for Septal Reconstruction Oral Mucosal Flaps for Septal Reconstruction
 Postauricular and Retroauricular Scalping Flap (The Paras Flap) Postauricular and Retroauricular Scalping Flap (The Paras Flap)
 Scapular and Parascapular Flaps Scapular and Parascapular Flaps
 Platysma Musculocutaneous Flap to The Lower Lip Platysma Musculocutaneous Flap to The Lower Lip
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|