Cheek Reconstruction With Tissue Expanders
John T. Stranix
Barry M. Zide
DEFINITION
Tissue expansion is a proven technique for generating additional cutaneous tissue to reconstruct facial defects when local coverage options are otherwise inadequate.
Skin adjacent to, or near, the surgical defect is stretched over time to produce adequate local tissue of similar color and texture for coverage without creation of a donor-site defect.
Expansion is achieved through placement of a buried prosthesis that is gradually filled with saline via a distant port.
As the volume of saline increases, the prosthesis enlarges and stretches the overlying tissue to cause expansion.
ANATOMY
Skin expansion results from mechanical stress applied over time through both mechanical creep (cellular stretch) and biologic creep (increased cellular proliferation).
Thickening of the epidermis occurs with concurrent thinning of the dermis and alignment of collagen fibrils.
Angiogenesis occurs in response to ischemia generated by tissue expansion, increasing both the number and caliber of blood vessels in the expanded tissue. This is similar to the increased vascularity seen with the delay phenomenon and expanded flaps can be considered delayed flaps.
Skin of the anterolateral neck shares essentially the same color, texture, and dermal appendages as the skin covering the majority of the cheek. This excellent match makes the neck an ideal donor site for cheek reconstruction with tissue expansion.
PATIENT HISTORY AND PHYSICAL FINDINGS
Tissue expansion is performed over 3 to 4 months, requiring office visits 5 to 7 days apart. This requires a motivated, well-informed, and compliant patient and family. Sometimes, twice-weekly fills can expedite expansion.
In some cases, parents and/or patients can do the fillings with proper instruction.
Tissue expansion has a higher complication rate in children compared to adults.1 Smokers also have an increased risk of complications.2
Facial tissue expansion must take into account the location, size, shape, and type of defect (nevus, burn, trauma, oncologic).
Expansion under scars or radiated tissue should not be done.
Consideration should be given to the aesthetic subunits involved, adjacent specialized structures that may be disrupted/distorted, skin quality, pre-existing scars, and any additional areas with reconstructive needs.
Available donor sites for expansion must be evaluated as this will determine the size and type of expander possible.
SURGICAL MANAGEMENT
The increased vascularity of expanded lateral cheek and neck tissue enables the design of unique advancement, rotation, or transposition flaps specific to individual cheek defects.
There are three general approaches to tissue expansion for coverage of cheek lesions:
Expansion of tissue immediately adjacent to the defect (which thins the skin)
Cervicofacial flap expansion and/or neck expansion for cervicofacial flap donor-site coverage
Direct expansion from below the lesion to allow excision and primary closure
An expander placed in the upper neck (as opposed to an expander placed immediately adjacent to the defect) is preferred because this approach results in decreased skin thinning.
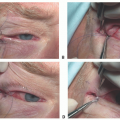
Transillumination of the expander in situ is a helpful technique because this approach identifies the major blood vessels of the flap by enabling the surgeon to perform back cuts more accurately.
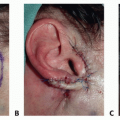
The Schrudde angle rotation flap adapts well to an expander placed in the neck. This flap incorporates an angular subcutaneous flap below the ear and backward. When the flap is brought up and forward, it fills the area in front of the ear, which would have a defect otherwise.
The size of the required expander can be calculated directly based on the length and width of the expected defect. When using a single expander, the length of the expander should be equal to or greater than the longest side of the lesion. The width of the expander should be the maximum possible according to anatomy.
The timing required to reach full expansion and the amount of fluid needed for expansion vary based on the quality and quantity of skin. Similarly, the timing of transfer after adequate fill has been obtained varies based on the condition of the skin and the amount of expansion that has been done. However, in general, once full expansion has been obtained, the transfer can be safely scheduled after 1 to 2 weeks.
Preoperative Planning
Careful flap planning should incorporate the expander placement incision(s) and align scars with borders of aesthetic units when feasible.
For large expanders, multiple access incisions may be required to allow for adequate expander pocket dissection.
Incisions are usually preauricular or open V shaped in the scalp or along the Schrudde infra-auricular incision.
If re-expansion and readvancement may be required for serial excisions, this should also be incorporated into flap choice and design. Serial expansions and excisions are associated with a higher extrusion rate during subsequent expansions.3 The author rarely re-expands the face.
Actual or anticipated defect size must be determined to select the appropriate number, size, and orientation of tissue expander(s). Location of remote port placement should be distant from the expander and secured in situ.
Donor-site selection plays an important role with the goal of providing a good soft tissue match in color, texture, and contour. For cheek reconstruction, the lateral cheek and neck provide an excellent match.
Positioning
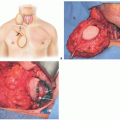
The procedure can be performed under sedation with monitored anesthesia care or full general anesthesia with the patient positioned supine on the operative table.
The head is turned toward the contralateral side from the defect, and the ipsilateral face, neck, and chest are prepped into the field.
Administration of an antibiotic with skin flora coverage 30 to 60 minutes prior to incision is recommended.
Approach
Size, shape, and number of the expanders
As stated earlier, in cases in which a single expander is used, the length of the expander should be longer than the length of the incision required to replace the intended area, whereas the width of the expander should be roughly equal to the width of the expected defect. In practice, we use the widest expander possible based on anatomic constraints.
Using the largest expander possible within the limitations of donor-site anatomy will reduce the number of expanders (and total expansion) required.
Compared to the expander base area, expander volume is less important due to the minimal risk of hyperinflation up to 10 times above the manufacturer’s stated nominal capacity.4
Using multiple expanders allows more rapid expansion with fewer complications than single expanders and should be considered when feasible.2
Soft, flat, rectangular silicone expanders with rounded corners are recommended for expansion of head and neck tissue. In the face and neck, floppy bag expanders are avoided due to knuckling and extrusion problems.
Port placement
Remote filling ports are preferred in the head and neck over integrated filling valves and are typically placed in the postauricular scalp or neck.
External filling valves may be helpful in children, but the port egress site must be dependent to allow for periprosthetic fluid drainage and should be far from the expander (greater than 6 cm) as they are associated with a higher infection risk.5
Ports must be secured to prevent drift.
Incision placement
Incisions for expander placement should not interfere with subsequent flap advancement or compromise the blood supply to the expanded tissue. Ideally, placement incisions are either incorporated into the subsequent flap design (like the Schrudde infra-auricular V), placed within the area to be excised, or distant like the scalp.
Access incisions should be kept away from the expansion process (greater than 2-3 cm) and never oriented parallel to expander edges as this increases exposure risk. Incisions should be either perpendicular to the expander or in the shape of a V or W with the broad base directed toward the expander.
Flap incisions and tissue transposition
Simply cutting around the advancing edge of the expander base does not take full advantage of the expanded tissue.
The following flap designs enable the most efficient use of expanded local tissue for coverage:
The single back-cut flap is ideal for triangular defects. The single back cut allows the flap to be advanced and/or transposed and is a workhorse technique. The flap can be shaped or contoured in a way to recreate a side burn or exactly tailored to a defect.
The double back-cut flap provides maximal gain of soft tissue advancement and is best for round or rectangular lesions. These flaps are amenable to re-expansion for serial excisions.
Over-the-top advancement flap allows for simple calculation of the amount of soft tissue available in the flap. This type of advancement is used when the expander was larger than the square-shaped defect. It does require sacrifice of some adjacent normal tissue over the lateral edges of the expander, and the required dog-ear excisions cause the flap to narrow when advanced.Related posts:
 Mandible Reconstruction With Fibula Flap With Templates
Mandible Reconstruction With Fibula Flap With Templates
 Lower Lip Reconstruction With the Nasolabial Flap
Lower Lip Reconstruction With the Nasolabial Flap
 Lateral Tarsal Strip Canthoplasty
Lateral Tarsal Strip Canthoplasty
 Reconstruction of the Ear Lobe
Reconstruction of the Ear Lobe
 Pectoralis Major Flap for Pharyngeal Reconstruction
Pectoralis Major Flap for Pharyngeal Reconstruction
 Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers
Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


