CHAPTER 17 Cheek–Midface Lift
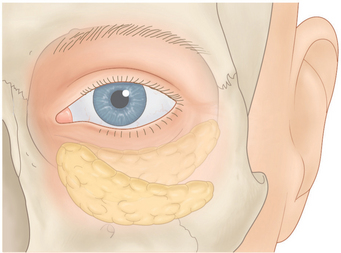
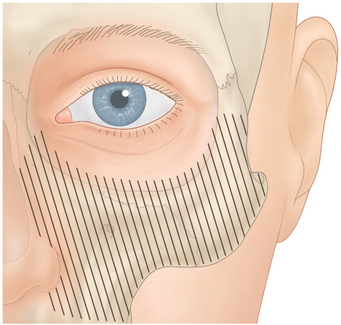
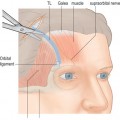
With age, the cheek migrates inferiorly and nasally (Fig. 17-1). This contributes to inferior orbital rim hollowing, a circle effect of the lower eyelids and cheek, a flattening of the cheek, cheek bags (festoons), and nasolabial fold. In the past, these problems have been treated with facelifts, excision of cheek bags, and cheek implants.
Hester and McCord1,2 popularized the cheek–midface lift through an external lower blepharoplasty approach. This procedure originally was done by reattaching the suborbicularis orbital fat (SOOF) in a more normal position along with a full thickness resection of the lower eyelid to stabilize the lid. The procedure has been modified multiple times and at present, I perform the procedure by suspending an orbicularis muscle flap along with tarsal strip and skin flap procedures. The operation places the ptotic cheek in a more normal position, relieves cheek bags, fills in the hollow inferior orbital rim with cheek fat, makes the midface more convex, and decreases the nasolabial fold depression. It also gives the effect of cheek implantation, adds skin to the lower eyelids for the treatment of cicatricial ectropion, and reduces the hollowing of the lower eyelid that sometimes occurs secondary to overzealous fat removal in lower blepharoplasty.
Surgical technique
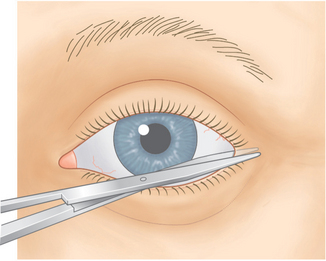
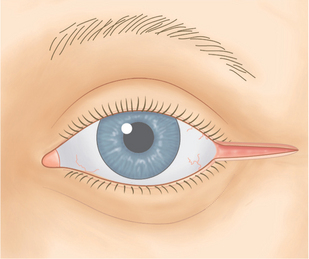
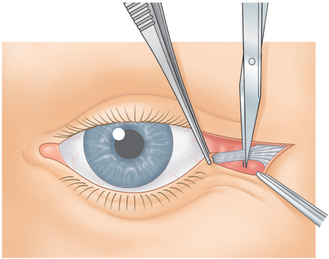
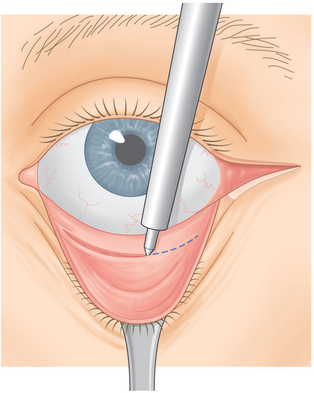
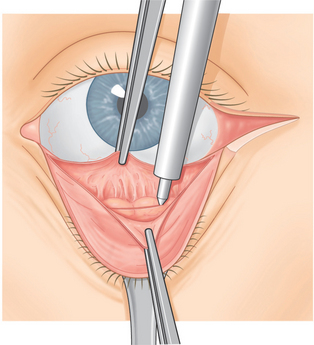
A #15 Bard-Parker blade is then used to make an incision through skin over the lateral canthal mark from the lateral canthus temporally in a horizontal direction for 1 to 1½ cm. A Westcott scissors is then used to sever the lateral canthus (Fig. 17-2). A Colorado needle then incises the orbicularis muscle from the lateral canthus throughout the length of the skin incision (Fig. 17-3). The lower limb of the lateral canthal tendon is severed (Fig. 17-4). A small Desmarres retractor everts the lower eyelid. One to two cubic centimeters of the anesthetic mixture is then injected subconjunctivally from the inferior tarsal border to the inferior fornix across the eyelid. The Colorado needle is then used to cut conjunctiva from the caruncle to the temporal aspect of the eyelid midway between the inferior tarsal border and the inferior fornix (Fig. 17-5). The surgeon grasps the central inferior edge of the severed palpebral conjunctiva while the assistant grasps the adjacent, more superior edge, with another forceps. The two forceps are pulled apart, and then the Colorado needle is applied across the eyelid between the two severed conjunctival layers through Müller’s muscle and capsulopalpebral fascia until fat is seen (Fig. 17-6).
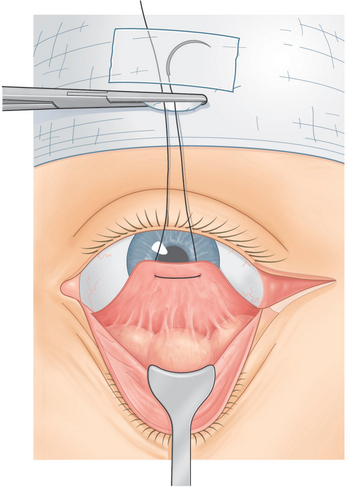
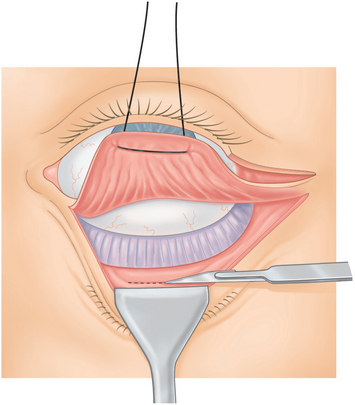
A 4-0 double arm black silk suture is passed through the inferior edge of conjunctiva, Müller’s muscle, and capsulopalpebral fascia with each suture arm. The sutures are then drawn upward and attached to the drape with a hemostat (Fig. 17-7). A small piece of tape is applied over any exposed needle to avoid needle sticks and to allow the suture to be reused, if needed. Usually the needle is cut and removed from the operating field.
The temporal herniated orbital fat is isolated, and the fat that prolapses with general pressure on the eye is clamped with a hemostat and cut along the hemostat with a #15 Bard-Parker blade (Fig. 17-8). Then cotton tip applicators are placed under the hemostat and a Bovie cautery is applied over the fat stump. The surgeon grasps the fat with the forceps before it is allowed to slide back into the orbit to make sure there is no residual bleeding that might cause a retrobulbar hemorrhage. After the first temporal fat pad is removed, the surgeon applies additional pressure to the eye to determine whether there is a second temporal fat pad.4 If found, it is removed in a similar manner.
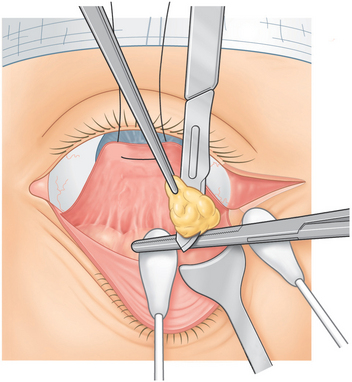
Figure 17-8 The surgeon removes the temporal orbital fat pad routinely and occasionally also the central and nasal orbital fat by cutting along the hemostat blade with a #15 Bard-Parker blade, and then applying a Bovie cautery over the fat stump. At times the nasal and central fat pads are repositioned (see Figs 17-22 & 17-23).
At times, the central and nasal fat pads are removed, and sometimes they are repositioned into the inferior orbital rim hollowing. This is a surgical judgement that is made depending on the severity and amount of orbital fat present preoperatively, as well as how much hollowing there is at the inferior orbital rim and nasal-jugal fold areas. If the decision is made to remove the fat, then the nasal and central orbital fat pads are removed in a similar manner to the description of the removal of the temporal fat pads. If the decision is made to reposition the nasal and central orbital fat pads, this is deferred until later in the procedure to avoid having to deal with the fat and sutures at this stage of the procedure.
Dissection of cheek periosteum
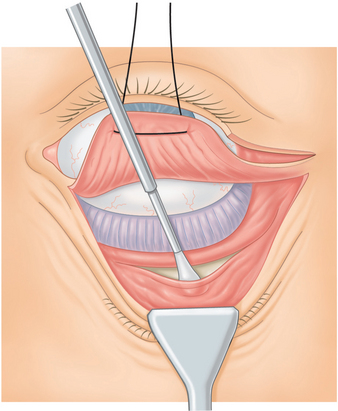
A medium size Desmarres retractor is used to retract conjunctiva, Müller’s muscle, and capsulopalpebral fascia over the inferior orbital rim. Using blunt dissection with a smooth end of a Tenzel periosteal elevator, the periosteum over the inferior orbital rim and lateral orbital rim are isolated. A Colorado needle or #15 Bard-Parker blade is used to incise periosteum several millimeters beneath the orbital rim from the nasal inferior orbital rim all the way across the orbit sweeping up into the lateral orbital rim (Fig. 17-9).
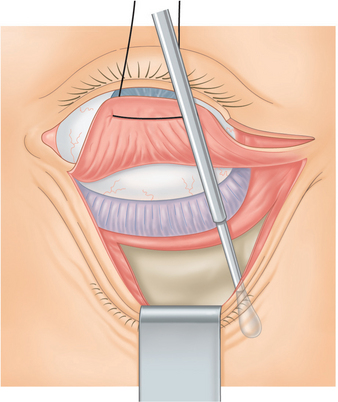
The sharp edge of the Tenzel periosteal elevator is used to reflect periosteum from the incision in a downward direction over the cheekbone (Figs 17-10 & 17-11). The surgeon should take care to avoid the area of the infraorbital foramen and nerve by palpating the inferior orbital foramen which was previously marked with a marking pen and by dissecting inferior to this position.
Most of the time, it is unnecessary to dissect periosteum nasal to the infraorbital canal; leaving periosteum nasal to the infraorbital nerve allows the nasal area to act as fulcrum for the cheek lift. However, if the purpose of the surgery is to add skin to the lower eyelid in the treatment of cicatricial ectropion or to reposition the nasal and central lower eyelid orbital fat pads, then dissection nasal to the infraorbital nerve is performed (Fig. 17-12).
During the periosteal dissection, small blood vessels such as the temporal zygomatic artery are commonly encountered; these are treated with the Colorado needle to coagulate these areas and thereby to avoid bleeding. Also should there be any bleeding from other areas of the cheekbone, the Colorado needle can be used to coagulate those, as well as in order to create a dry field.
Related posts:
 Upper Blepharoplasty Combined with Levator Aponeurosis Repair
Upper Blepharoplasty Combined with Levator Aponeurosis Repair
 Evaluation of the Cosmetic Oculoplastic Surgery Patient
Evaluation of the Cosmetic Oculoplastic Surgery Patient
 Brow Lift Techniques
Brow Lift Techniques
 Treatment of Lower Eyelid Dermatochalasis, Herniated Orbital Fat, and Hypertrophic Orbicularis Muscle
Treatment of Lower Eyelid Dermatochalasis, Herniated Orbital Fat, and Hypertrophic Orbicularis Muscle
 Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
 Injectable Agents for Dermal Soft-Tissue Augmentation of the Face: Options and Decision Making
Injectable Agents for Dermal Soft-Tissue Augmentation of the Face: Options and Decision Making
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


