CHAPTER 45 Laser and Energy-Based Treatments in Men
Summary
This chapter details common cosmetic applications of lasers and related therapies in men. These include laser hair removal, tattoo removal, and treatments for rosacea, sun damage, and acne scarring. Nonsurgical skin tightening and nonsurgical fat reduction and body contouring are also covered. Gender-specific anatomy, cutaneous physiology, diseases, and treatment goals are important considerations when selecting treatment for the male patient. Approaches described in this chapter are likely to be in high demand among male cosmetic patients who comprise an increasing portion of the nonsurgical cosmetics market.
Introduction
In 2015, the number of both surgical and nonsurgical cosmetic procedures continued to rise, with a total of approximately 13,000,000 procedures performed. This corresponds to a 39% increase over the past 4 years. 1 Within this boom, nonsurgical or minimally invasive procedures have significantly outpaced surgical approaches. Nonsurgical procedures have increased 44% over the past 5 years, compared to 17% for surgical procedures, with laser and laser-related technologies accounting for a substantial portion of these figures. 1
Though traditionally sought by mostly female patients, such cosmetic procedures are in increasing demand among male patients. Although men represented only about 10% of cosmetic dermatology patients, the last 20 years has seen an increase of over 300% in the number of cosmetic procedures performed on men. 1 , 2 Data from the American Society of Plastic Surgeons shows a substantial increase between 2014 and 2015 in the number of men undergoing nonsurgical, laser-based skin rejuvenation, hair removal, fat removal, and tattoo removal. 1
The minimally invasive nature, subtle results, and minimal downtime of most laser- and light-based therapies make it an appealing modality for male patients, who tend to be more conservative than their female counterparts with regard to cosmetic procedures. 3 Laser therapy is also attractive to men because there is less of a risk of feminizing the face, as can be seen with injectables. Increasing awareness of available procedures and social acceptability of cosmetic procedures among men also contribute to the uptick.
With the increasing proportion of male cosmetics patients, it will be important that practitioners recognize the distinct anatomy, cutaneous physiology, and treatment goals of this demographic. This chapter will review these topics as they apply to laserand light-based therapies and also detail the array of other available energy-based technologies currently in use.
Anatomy and Cutaneous Physiology in Men
The skin is highly influenced by and actively metabolizes sex hormones including estrogen and testosterone. Differences in the levels of sex hormones in the skin of men as compared to women contribute to gender differences in cutaneous physiology and microstructure of the skin. 4 , 5 These differences must be considered when using energy-based skin procedures on men.
The male face has thicker skin (both epidermis and dermis) and a greater density of dermal collagen than in women. 5 However, men have less subcutaneous adipose tissue, which, along with larger stronger muscles of facial expression, contributes to more prominent rhytides compared with females. 2 , 6 Studies confirm that at any given age, male patients appear older than similarly aged female patients. 7 , 8 , 9
Larger, stronger muscles and increased skin thickness mean that men may require higher doses of light energy to achieve a given cosmetic result. It also means they may be more likely to tolerate higher doses. Green and colleagues noted that men have less edema and erythema than women after fractional nonablative therapy 3 ; we have noticed the same. One study also suggested that more tattoo treatments are needed for men compared with women, 10 though we have not noticed this in our practice. Anecdotally, male patients also seem to seek treatment at a later stage than females, who are more amenable to preventative measures.
Additionally, Doppler studies have demonstrated greater facial arterial blood flow in men when compared with age-matched women. 11 This is perhaps related to dense terminal hair and their associated blood supply. 12 Men have a greater density of coarse terminal hair not only on the face but also on the trunk and extremities. 13 As a result of increased cutaneous vascular supply, some studies have demonstrated more bruising in male patients following laser procedures. 14
Practitioners should also be aware that a higher density of terminal hair may lead to inadvertent destruction of facial hair during laser treatment of other targets over the face and neck. Care must be taken in these areas to be cautious with long pulse durations and monitor for perifollicular erythema, which may be a sign of follicle damage.
In addition to increased hair density and collagen thickness, male facial skin also has a higher density of eccrine and sebaceous glands. These appendages show greater activity in men, secreting more sweat and sebum than in females. 4 More active and densely positioned sebaceous glands may explain the greater incidence of rhinophyma in male patients. 15
Finally, subcutaneous fat distribution differs among men and women with men tending to develop subcutaneous fat deposits over the central abdomen and chest. Women in contrast develop more subcutaneous fat over the buttocks and thighs. 16 Many men develop increased visceral fat that may lead to abdominal protuberance and cannot be targeted by invasive or noninvasive approaches.
The above variations in anatomy and physiology, in addition to various psychosocial factors discussed above, impose a set of unique clinical considerations when caring for male cosmetic patients.
Common Cosmetic Applications of Laser and Related Therapies in Men
Laser Hair Removal
Laser hair removal is among the most popular and rapidly growing cosmetic procedures among men. In 2015, 130,142 men underwent laser hair removal, 1 an increase influenced by shifting perceptions of male body hair and increased awareness of available treatments. 2 The most commonly treated areas include the beard area, chest, back, and upper arms. 17
Laser hair removal relies on selective photothermolysis of melanin in the hair shaft. As the chromophore absorbs these targeted photons, they are converted to heat. When delivered at long pulse durations, this heat is propagated to and causes thermal injury to the hair bulge and bulb. 18 , 19 Numerous techniques exist to remove unwanted hair but laser hair removal offers a fast, well tolerated, and permanent approach.
Melanin exhibits a strong absorption peak from approximately 400 to 1,000 nm. 20 At the lower end of this spectrum, melanin absorption is sufficiently high that epidermal damage and resultant scarring or dyspigmentation becomes a risk for patients with dark skin. 19 Relative sparing of the epidermis can be achieved at the longer visible and near-infrared wavelengths, which penetrate more deeply. However, the ability to treat lighter hair, which is less dense with chromophore, diminishes at these higher wavelengths. 19 , 21
Several types of lasers and light devices have been used for hair removal and each may offer benefits and drawbacks depending on the characteristics of the patient being treated. The ruby, alexandrite, diode, neodymium yttrium aluminum garnet (Nd:YAG), and intense pulsed light have all been demonstrated safe and effective modalities in laser depilation in men. 21 Though rarely used for hair removal today, the ruby laser, operating at a wavelength of 694 nm, has been shown to yield hair clearance of up to 20% to 60% following a single treatment. 22 , 23 As with the alexandrite laser, discussed below, there is concern that the shorter wavelength of this laser may target epidermal melanin in patients with darker skin leading to burns, hyperpigmentation, or hypopigmentation. 23
The alexandrite laser is commonly utilized for laser hair removal in patients with lighter complexions (Fitzpatrick skin types, FST 1–3). 24 At a wavelength of 755 nm, there can be targeting of epidermal melanin with a theoretical risk of resultant dyspigmentation in patients with darker skin. However, more recent studies have demonstrated the alexandrite laser to be safe for use in patients with FST 4 to 6, with complications occurring in only 2% of cases when using long pulse durations. 25 However, patients with type 6 skin had a significantly higher incidence of adverse events and the alexandrite laser is best avoided in this population. 25 Because this laser strongly targets melanin, it can be helpful for the treatment of finer vellus hair that is much less densely pigmented. 26
The Nd:YAG laser (1,064 nm) remains a safe and well-tested approach to hair removal in patients with all skin types including FST 4 to 6. 23 The 1,064-nm wavelength penetrates deeper and targets melanin slightly less avidly, providing some epidermal protection. Because of this, the risk of hypopigmentation in dark skin is much less than with the alexandrite or ruby lasers. 23 A recent study by our group investigated treating patients with FST 3 to 6 skin using the Nd:YAG laser and had no incidents of dyspigmentation, scarring, or other long-term complications. 27
There is limited data directly comparing the efficacy of various lasers, and different parameters (pulse duration, fluence, and spot size) are used in different studies. However, several clinical studies do directly compare the ruby, alexandrite, and Nd:Yag, 22 , 23 , 28 and results tend to show that ruby and alexandrite lasers are more effective in hair removal, while the Nd:YAG produces the lowest incidents of adverse events.
Intense pulsed light devices emit light containing a broad band of wavelengths (590–1,200 nm) that can excite multiple chromophores. 29 The wavelengths emitted can be selected based on the patient’s skin type as well as the chromophore being targeted. 21 Longer wavelengths and a greater number of pulses per sequence are used in darker skin tones. 30 The need for cooling gel, direct contact of probe with skin, and lack of perifollicular erythema as a clinical end point makes this device more cumbersome to use for hair removal. It is not safe for darker skin types, and the risk of burn is relatively high.
In recent years the diode laser has gained popularity in laser hair removal and this technology may be useful in treating patients requesting treatment of large areas of skin such as the chest and back as commonly requested by men. This 810-nm laser has been demonstrated in clinical trials to perform favorably compared with other lasers used in hair removal. 31 , 32
New versions of the diode laser utilize large treatment zones, rapid short pulse durations, and low energy fluence to provide a more comfortable and faster procedure while maintaining efficacy. New devices also utilize negative pressure at the device head to stretch the skin, reducing hair density and thereby the amount of energy required for photolysis of hair. Additionally, the diode laser has been shown to be safe for use in patients with darker skin tones. 33 Campos and colleagues have reported that hair on the face seems to respond better to diode laser than those on the body. 31
Treatment of pseudofolliculitis barbae (PFB) is an important therapeutic application of laser hair removal in male patients. PFB is a common inflammatory follicular disorder in individuals with thick curly hair. Plucking or close shaving leads to ingrown hair that induce a foreign body type inflammatory response. The primary presentation of PFB is erythematous papules and pustules in the beard or other terminal hair-bearing areas. When chronic inflammation is present, hyperpigmentation, hypopigmentation, and fibrotic scarring can occur, which can be cosmetically disfiguring. 34 Acne keloidalis nuchae (AKN) is a similar process occurring on the occipital scalp and posterior neck that ultimately results in keloidal papules and plaques. 35 Adjustment of shaving habits and use of topical medications often fail to adequately manage these conditions, especially among patients who must continue to shave for social or professional reasons. Laser hair removal can therefore be considered for more effective and permanent treatment.
Both PFB and AKN are much more common in patients with darker skin tones, making hair removal somewhat more challenging. Long wavelength light in the near infrared spectrum, namely 1,064-nm light, is therefore preferred to protect epidermal pigment. Multiple studies have demonstrated decreased incidence of papules and pustules as well as a reduction in scarring and hyperpigmentation with use of the Nd:YAG. 36 Recent studies also confirmed that the diode laser is safe and effective for improving PFB as well as AKN in patients with skin phototypes 1 to 4. 37 , 38
Tattoo Removal
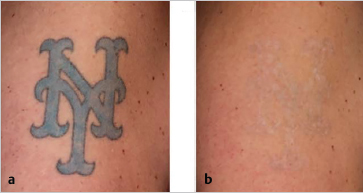
Between 2014 and 2015 the number of men seeking laser tattoo removal increased almost 50% from around 8,000 in 2014 to about 15,000 in 2015. 1 The recent development of picosecond laser technology has increased the effectiveness and decreased the number of treatments needed for tattoo removal compared to traditional nanosecond Q-switched technology 39 ( Fig. 45.1 ). Laser tattoo removal is believed to work by the same principle of photothermolysis whereby particles of tattoo pigment absorb light energy according to their chemical absorption peak. The absorbed energy causes a dramatic increase in temperature of the tattoo particle inducing fragmentation. Photoacoustic fragmentation also plays a role, especially with picosecond devices. 40 , 41 This occurs when very short pulse durations create acoustic waves within the surrounding tissue, which further fracture and fragment pigment particles. Once fragmented into smaller particles, tattoo pigment is cleared by the reticuloendothelial system. 41
The type of laser used for tattoo removal depends on the color of the targeted pigment. The most commonly used wavelengths of light for tattoo removal are as follows:
5 nm (alexandrite) for treating black, green, blue, and violet.
1,064 nm (Nd:YAG) for treating black and other dark colors (especially in darker skin).
2 nm (frequency-doubled Nd:YAG) for treating red, orange, and yellow.
t (ruby) for treating black, green, blue, and violet.
Two recent studies by our group have demonstrated the unique benefits of picosecond laser technology in the treatment of tattoos containing blue, green, and yellow inks. 42 , 43 Such pigment colors have classically been more recalcitrant to treatment with older Q-switched laser technology. In one study, a 755-nm picosecond pulse duration laser was used to treat blue and/or green pigment-containing tattoos, including untreated and previously treated tattoos. All treated tattoos had between 75% and 100% clearance after only one or two treatment sessions. There were no incidents of scarring or residual pigmentary alteration on follow-up. 42 Similar results were obtained in yellow pigmentcontaining tattoos with the use of a frequency-doubled 532-nm Nd:YAG picosecond laser. 43
Photorejuvenation
Laser- and light-based modalities have been used in the treatment of rhytides, dyspigmentation, and photoaging since the 1980s. Laser resurfacing can broadly be categorized as ablative (full thickness destruction of the epidermis) or nonablative, and ablative can be further defined as either fractionated or nonfractionated. Tissue water is the most commonly targeted chromophore in laser photorejuvenation to target both epidermal keratinocytes as well as dermal collagen and vasculature. Intense pulsed light may also be used, which consists of a broad band of light targeting both hemoglobin and melanin at once.
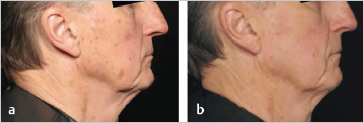
A popular treatment for men in our practice is the fractional nonablative 1,927-nm thulium laser (Fraxel Dual, Valeant, Bridgewater, NJ). Not only has this laser demonstrated improvement in the appearance of rough skin, skin tone, pores, and pigment, but it also has proven efficacy for actinic keratoses 44 ( Fig. 45.2 ). This is therefore a cosmetically elegant treatment for men with actinic field disease, especially compared with other traditional therapies such as topical chemotherapy and photodynamic therapy. Men may be more likely than women to have significant actinic damage on the face given that they are likely to have used less sunprotective creams or makeup in the course of their lives. 45 Fair-skinned men with patterned baldness may have significant field disease on the scalp as well, where nonablative fractional resurfacing is also likely to be beneficial.
Men may also seek cosmetic rejuvenation for roughness, erythema, and dyspigmentation associated with photodamage. The nonablative 1,927-nm thulium is ideal for men as it is a fast procedure with subtle results and minimal downtime. Increased redness, mild swelling, and dry scale is present for about 4 to 5 days. 46 The nonablative 1,550-nm erbium-glass option (Fraxel Dual, Valeant, Bridgewater, NJ) is slightly stronger and deeper and also appropriate for rejuvenation.
For those men who wish to target rhytides or skin laxity, deeper resurfacing with fractional ablative therapy is available, for example, with the carbon dioxide laser. However, full thickness destruction of the epidermis leads to prolonged recovery time, with wounding of the skin that takes 7 to 10 days to heal, and subsequent erythema that lasts up to 2 months. 47 These effects, especially prolonged erythema, are especially challenging in male patients who do not typically wear camouflage makeup and may feel more stigmatized for having had a cosmetic procedure. Some physicians like to incorporate 590-nm lightemitting diodes light posttreatment to reduce erythema, especially in men. 3 Any resurfacing procedures should be done with caution in skin type 4 or higher because of risk of pigment gain or loss. 48
Intense pulsed light is also used for photorejuvenation and remains a possible noninvasive approach. Because it is a broad band of light, it targets both “reds and browns” and can be an excellent choice for poikiloderma. Though less effective than more targeted treatment with laser, it may be attractive to men who appreciate the lack of need for anesthesia and ease of a “two-for-one” approach for both dyschromia and erythema. As a tradeoff, four to six sessions may be required for optimal results while noticeable results are often seen after only one fractional laser session. It has not been shown to be beneficial for actinic keratoses such as fractional nonablative treatment.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


