CHAPTER 44 Kybella
Summary
Kybella (deoxycholic acid) is an FDA-approved lipolytic agent used to treat unwanted submental fullness. Proper injection technique is paramount to successful treatment for efficacy but more importantly to ensure safety as risks including temporary paralysis of the marginal mandibular nerve can occur. This chapter will include the history that led to the innovation of Kybella as well as a review of the anatomy of the submental area. Illustrations and photographs of the tools and steps recommended for the proper injection technique will accompany this chapter, as well as an instructional video.
Introduction
Fat reduction has traditionally been performed by surgical means, including excision as in an abdominoplasty, or with more targeted approaches such as with liposuction. Fortunately, as our understanding of adipose tissue has improved alongside advances in technology, less invasive approaches have become safer and more effective. While many successful face and neck lift procedures, such as platysmaplasty, as well as liposuction cases have been performed, the anatomy of the submental fat pad presents unique challenges that make a minimally or noninvasive approach much more favorable.
Taking advantage of appropriately cold temperatures and duration of exposure, CoolSculpting by Zeltiq has demonstrated successful reduction of subcutaneous fat of the trunk and extremities for over a decade, and most recently developed an applicator for treatment of submental fat. Utilizing a prototype device, 60 subjects with unwanted submental fat underwent a 60-minute treatment, with an optional second session 6 weeks later. Blinded assessment was performed by review of photography (determined before and after), ultrasound, and patient questionnaire at 3 months after last treatment. Ultrasound measurements found an average reduction of 2 mm in fat, with 77% of subjects reporting reduction in visible fat and improvement in appearance. At present, the commercially available device is a 45-minute session, repeated 1 month apart. Additionally, treatment approach continues to be modified with many advocating use of an overlap instead of direct treatment of the peak area of concern. Furthermore, although CoolSculpting delivers results, not all patients may be candidates. For example, patients with a narrow submental area or those with minimal amounts of submental fat may be more difficult to treat with this modality.
The promise of an effective injectable agent for the reduction or removal of fat is one that has eluded individuals—patients and physicians alike—for decades. Termed mesotherapy, the practice of superficial injections of various agents for the treatment of pain was first described by the French physician Michel Pistor in the 1950s. In treatment of tissues specifically derived from embryonic mesoderm, in addition to providing cure, the intent of these local injections was to avoid the need for systemic administration. Indications for this technique continued to expand—particularly in Europe, and most recently has been employed in treatment of additional cosmetic concerns. An important distinction made by Rotunda and colleagues is in the treatment of localized fat and cellulite, where subcutaneous injections of a combination of phosphatidylcholine, a cell membrane component, and its solvent sodium deoxycholate, have been investigated for this purpose with some reported success. They noted that these are not among the impressive list of medicines, herbal compounds, and others that are combined in more commonly administered traditional mesotherapy formulations of Europe. However, the injection of these two agents—or at least one—seems to hold the most potential as an injectable lipolytic agent. Just over a decade ago, it was determined that in fact the deoxycholic acid solvent was just as potent a lipolytic agent as the main ingredient. Furthermore, studies into the bile salt in the treatment of unwanted submental fat resulted in the formulation that has come to be known as ATX-101, or Kybella. This nonanimal, nonhuman formulation results in lysis of adipocytes when injected into the subcutaneous fat. Cell membrane disruption then results in an inflammatory response involving phagocytosis by macrophages as well as recruitment in fibroblasts and resultant neocollagenesis.
The “double chin” describes the loss of definition of the cervicomental angle as a result of an enlarged submental fat pad—a distinct compartment within preplatysmal fat. In a randomized, double-blind, placebo-controlled phase 3 trial, subjects received up to six treatments with ATX-101 or placebo spaced approximately 4 weeks apart. A statistically significant greater reduction in submental volume in the treatment group was observed by both caliper and magnetic resonance imaging. Of interest, despite this reduction, skin laxity was either unchanged or improved in most subjects. This is consistent with a local tissue response described above that includes neocollagenesis. These results have been maintained in long-term follow-up of subjects from the company’s phase 2 trials as far out as 4 years. The most common side effects reported included edema, bruising, pain, and numbness.
In this chapter, we will discuss the use of Kybella in the treatment of unwanted submental fullness, with a special focus on the treatment of men.
Physical Evaluation
While evaluating the patient, palpate the submental area to ensure that the patient is a good candidate for treatment.
Ask the patient to make a face to tense the platysma (show the lower teeth) to help identify the subcutaneous fat between the dermis and preplatysmal fat.
Have the patient smile to observe any asymmetries as the marginal mandibular nerve affects the corners of the mouth.
Ensure the patient has no active skin infections in the area to be treated.
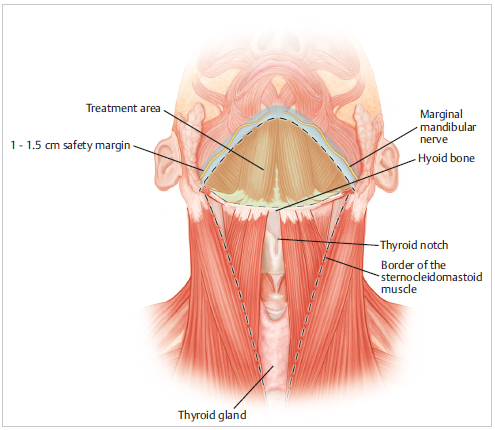
Identify anatomical structures: sternocleidomastoid muscle, hyoid bone, which will form the lateral and inferior borders, respectively.
Anatomy
Loss of definition of the submental area is in many cases a direct result of weight gain; however, many individuals of ideal body weight may also have what is commonly referred to as a “double chin.” This prominence of a submental fat pad could be the direct result of lifestyle (diet and exercise), and also secondary to a combination of genetics and anatomy of this area of the head and neck as we age. While Kybella is only intended to treat the prominent submental fat, we will review the anatomy of this area in its entirety as it relates to the appearance and structure of the chin and neck ( Fig. 44.1 ). An understanding of this anatomy is not only necessary in governing how we properly assess and approach our Kybella treatment, but also will allow the physician and patient to better understand what effects reduction of the fat pad may have on the area in general. Of importance, there is the potential for the revealing of skin laxity and jowls, or prominent platysmal bands that were less obvious or evident prior to treatment.
The lower face is defined by the chin, which is the fusion of two bones during human development to constitute the mandible. This facial bone is what forms the lower jaw and contains the lower teeth. Bony landmarks to consider during treatment include the horseshoe-shaped anteriormost aspect of the mandible—the corpus mandibulae and the foramen mentale, which can be palpated and located below the second premolar. Inferiorly, it is important to identify the thyroid cartilage and hyoid bone in the midline of the anterior neck. With aging come changes in the facial skeleton overall and selective resorption of bony support of the midface as well as prejowl area of the mandible, resulting in the downward motion of overlying tissues and loss of definition of the lower face.
Directly below the skin of the chin lies the submental fat, which is compartmentalized into central, medial, and lateral fat pads. Furthermore, these collections of fat are situated in both pre- and postplatysmal planes. As with liposuction, treatment with Kybella only targets the preplatysmal fat. The platysma muscles arise from the muscles of the chest and shoulder and insert into the lower mandible, risorius, and paired contralateral platysmal muscle, directly continuing into the facial superficial musculoaponeurotic system (SMAS). Therefore, this broad superficial muscle can be found throughout the area of the chin and neck, serving to protect the underlying muscles, arteries, veins, and nerves.
The mental neurovascular bundle can be found along the midpupillary line at the mental foramen. As the facial artery branches from the external carotid and emerges from the submandibular gland, it divides to form the submental artery, which passes over the body of the mandible and branches into superficial and deep components. This artery anastomoses with labial and mental arteries. The mental artery arises from the inferior alveolar branch of the maxillary artery after traveling through the mandibular canal, emerging with its respective nerve and supplying the chin. The inferior alveolar artery is a branch of the mandibular division of the larger of the two terminal external carotid artery branches, the maxillary artery. This artery originates within the parotid gland, at the mandibular level of the neck, and is divided into three segments: mandibular, pterygoid, and pterygopalatine.
The mental nerve provides sensory innervation to the lip and chin and forms from the inferior alveolar nerve at the mental foramen of the mandibular canal. The mental foramen in located 2.5 cm lateral to the midline, in the same plane as the supraorbital and infraorbital foramina. The inferior alveolar and mental nerves supply the lower teeth and lip and chin. The lingual nerve is a branch of the mandibular nerve that crosses the duct of the submandibular gland to reach the tip of the tongue. It receives sensory input from the anterior two-thirds of the tongue. Motor innervation to the lower face and upper platysma is provided by the marginal mandibular branch of the facial nerve. It is important to recognize that as it crosses the mandible, the marginal mandibular nerve is covered only by platysma and skin and is vulnerable to injury. The remainder of the platysma is innervated by the cervical branch.
The marginal mandibular nerve courses approximately 1 to 2 cm below the inferior border of the mandible. Anatomical variations do occur and it has been reported to be found up to 4 cm below this landmark. The marginal mandibular nerve can be affected inadvertently with neuromodulators as well as deoxycholic acid. Injury from other sources, including trauma can also occur, which can manifest as transient or permanent paresis. The depressor muscles, which are innervated by this nerve, can fail to contract, most commonly observed when a patient smiles, demonstrating asymmetry.
There are both obvious and subtle differences in male and female anatomy; among them are differences in hair distribution, muscle mass, and skeletal size ( Fig. 44.2 ). Regarding the latter, the male skull is larger with a more square shape and wide-angled jaw compared to a woman’s more gradual taper from upper to lower face. Specifically, among the most commonly perceived features of a “masculine face” are strong mandible, including a prominent jaw and chin. Further definition of the male jaw and chin is provided by larger masseter muscles. There is a greater density of blood vessels in the male face than in the female face. A Doppler perfusion study demonstrated greater blood flow in men compared to women, mainly because of a greater number of microvessels present. This may be related to the presence of coarse facial hair. A dense vascular plexus supports individual hair follicles, and thicker hairs tend to have more capillaries supplying the dermal papilla. Consequently, men are more prone to bruising after injections as well as postoperative bleeding following facial surgery in general.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


