CHAPTER 40 Body Lift after Massive Weight Loss in Men
Summary
After massive weight loss, men seek body-contouring surgery to correct gynecomastia, remove unsightly bulges, and tighten loose skin. In this chapter, the reader will learn the planning and execution for the removal of excess skin and fat, along with improving masculinity. Our operative design is an innovative crisscross pattern of elliptical excisions across the torso that essentially removes both horizontal and vertical excess skin. Lipoabdominoplasty is extended through oblique flank excisions that diminishes the lower body and is combined with excision of the gynecomastia and an upper body lift that raises the nipple–areolar complex, obliterates breasts and inframammary fold, and leaves tight skin-wrapped superficial muscles. Comprehensive excisional body-contouring surgery of a central high-tension abdominoplasty with a series of obliquely oriented ellipses throughout the torso appears to provide low-risk improved body contour for the muscular male.
Introduction
After massive weight loss (MWL), men seek body-contouring surgery to correct gynecomastia, remove unsightly bulges, and tighten loose skin. Many also would like upper body dominance and muscular show. Unfortunately, these features are unlikely to be fully restored after traditional correction of gynecomastia and abdominoplasty with a lower body lift. With the planning and execution presented here, excess skin and fat can be removed along with improving masculinity. Our operative design is an innovative crisscross pattern of elliptical excisions across the torso that essentially remove both horizontal and vertical excess skin. Lipoabdominoplasty is extended through oblique flank excisions that diminish the lower body and is combined with excision of the gynecomastia and an upper body lift that raises the nipple–areolar complex (NAC), obliterates breasts and inframammary fold (IMF), and leaves tight skin-wrapped superficial muscles.
In contrast, shapely women desire bodycontouring surgery that removes loose skin leaving sculptured adipose-related features with lower torso dominance. Round high breasts should dominate narrow chest and shoulders. A tight, narrow waist and slightly rounded lower abdomen should abruptly expand to full hips and rounded buttocks that are wider than the shoulder span. Bodycontouring literature is replete with techniques to enhance feminine contours with relatively little attention to the male physique.
Physical Evaluation
Assess general excess skin and adipose of the trunk.
Assess extent of gynecomastia.
Assess flank bulging.
Assess buttock ptosis and atrophy.
Assess pectoralis, latissimus dorsi, rectus abdominus, and external oblique development.
Assess the tissues remaining after a total body lift to determine whether upper body dominance and muscular show can be achieved. If not, further weight loss or extensive liposuction is recommended.
Access upper arm excess skin and fat from elbows to across axilla.
Access excess skin and adipose of thighs.
Anatomy
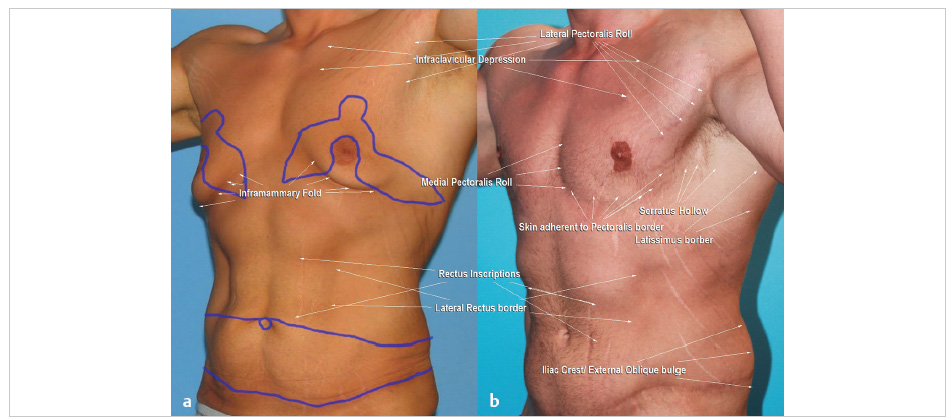
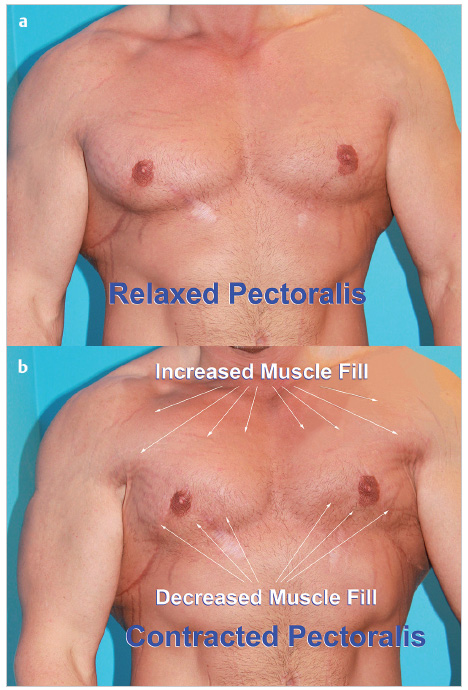
Surgically relevant aesthetics starts with an appreciation of dominant broad shoulders and rib cage draped with bulging sheets of contoured muscles that taper to a narrow waist highlighted by a six-pack abdomen and narrow rounded buttocks ( Fig. 40.1a ). Our muscular model is a 5 foot 10 inch, 185-pound part-time fighter. Three years earlier, he had lost 100 pounds followed by boomerang pattern correction of gynecomastia extended with a short transverse upper body lift, and an abdominoplasty extended with a transverse lower body lift ( Fig. 40.1b ). There is heightened muscular show covered with faded scars on the chest and lower torso. Replacement of the gynecomastia and loose chest skin reveals subtle contours of the pectoral muscle that change with arm position and active contraction ( Fig. 40.2 ).
Obviously female breasts obscure the dynamics of relatively small pectoralis muscles. The inferior and lateral borders of the pectoralis muscles are defined about the fourth and fifth ribs. A recess of intercostal and serratus muscles is seen rippling between the prominent lateral borders of the pectoralis and latissimus dorsi muscles. A flat rectus abdominus muscle, indented by two transverse inscriptions, extends from costal margin to mons pubis. The rectus muscles are further contoured by narrow depressions along the midline linea alba and obliquely oriented lateral rectus border. Reduced waists swell to the hips. The external oblique muscle smoothly rounds above the prominent iliac crest. Unseen are the narrow and rounded buttocks.
Men obsessed by their muscular appearance are aware of these contour subtleties and dynamics, and welcome relevant observations by their plastic surgeon. The most effective total body lift combines boomerang correction of gynecomastia and J torsoplasty upper body lift (Chapter 22) with an abdominoplasty extended by oblique flankplasties.
A thorough reduction of bulky lower torso diminishes its bearing on overall torso shape, allowing upper torso dominance. When coupled with effective brachioplasties, the aesthetic impact is greater. Further benefit of these complimentary oblique excisions of the back and plastic closures is improved definition of the superior iliac crests, posterior costal margins, and latissimus dorsi and external oblique muscles.
For the upper torso to dominate the lower, bulging pannus, flanks, and hips must be dramatically reduced and aggressive liposuction applied to the abdominoplasty. Remove loose skin through a complete abdominoplasty using adequate liposuction of the epigastrium or vertical midline excision as needed. While liposuction of the flanks helps, oblique excision of flank bulges is the only reliable means to narrow a waist in this patient population. A tight closure along the flank in concert with the abdominoplasty and J torsoplasty tapers the body from costal margin to iliac crests. The common adverse lower body lift sequela of retained flank bulges and lateral gluteal depression is completely avoided. While the lateral buttocks are lifted, the rising central gluteal crease cannot occur because the lower posterior midline is untouched.
Patient Selection
Lipoabdominoplasty with oblique flankplasties and crisscrossing upper body lift leave a tight skin envelop over well-developed muscles and a smaller lower torso. This complex operation is best suited for moderate-to-severe deformity in men willing to accept long scars not covered by underpants. Nevertheless, since the long bilateral anterior chest closures encircle each superior border of the NAC, there is an aesthetic interruption of the scar. Continuation through a lateral J torsoplasty hides that body lift scar under the resting arm. Oblique scars along the flanks and lateral chest routinely heal fine; however, prolonged persistent hypertrophy of the medial chest scar is a risk. The more commonly performed traditional hip hugging lower body lift may be patient preferred because of the scar position hidden by underwear, although postoperative elevation of the central buttock crease is problematic. The concern over medial chest scar hypertrophy is a reason for which otherwise suitable candidates decline boomerang pattern correction. Obliquely oriented closures over the anterior lateral chest uniformly are considered the most aesthetic for correction of gynecomastia.
Mild-to-moderate gynecomastia without chest laxity is best treated with ultrasound-assisted liposuction of anterior chest with glandular pull through resection along a periareolar incision. Recently, moderate gynecomastia with ptosis is being corrected without any incision with minimally invasive controlled bipolar radiofrequency energy through BodyTite (InMode, Tel Aviv, Israel) with promising results. At extreme NAC ptosis, the boomerang or J torsoplasty operation may not work because the skin is too loose to remove all the gynecomastia and epigastric excess while transposing the NAC a relatively short distance. Operations more focused on gynecomastia, perhaps with NAC skin grafting, would be indicated.
Midchest transverse excisions mostly remove vertical excess. The residual horizontal redundancy of skin leaves laxity that obscures muscular detail and disappointedly hangs when leaning over. An inferior buried pedicle flap to vascularize the NAC leaves too much inferior fullness. That thickness is most noticeable when the pectoralis muscle is contracting or on stretch, which should leave that area empty ( Fig. 40.2 ). A long transverse excision that may have to cross the sternum and positioned along the prior IMF, usually creates a new IMF. That undesirable female type adherence is most evident when leaning over.
This demanding surgery is scheduled no sooner than 1 year after weight loss is stable. The anticipated residual subcutaneous tissue needs to be thin enough to reflect underlying muscle. If that has not been achieved, then further weight loss or focused liposuction is necessary. The patient needs to be physically fit with good nutrition as determined by history, physical examination, and screening laboratory tests.
While the lower and upper body surgery may be operated on separately, they are probably best planned in consideration of the other, as each excision closure interrelates to achieve an overall tight skin envelope and obliteration of the IMF.
Steps for Total Body Lift
The case example is presented in Video 40.1 and in all these steps. Four preoperative views show the surgical markings of a single-stage total body lift ( Fig. 40.3 ). In summary, the abdominoplasty with its lateral extensions directly over the bulging flanks is drawn first while standing. The elliptical extensions ascend posteriorly from the iliac crests. The width of excision is determined by invagination of the flank roll. The upper body lift with boomerang correction with its J torsoplasty upper body is drawn next while taking care to limit superior distraction of the abdominoplasty and flank resection lines. L brachioplasties and/or spiral thighplasties may be added to the torso plan.

The surgical marking starts with a perpendicular connecting the sternal notch to the midpubic tubercle. Any lateral deviation of the central umbilicus is noted. A roughly 12-cm-long suprapubic horizontal line is centered on the pubis from 6- to 9 cm from the base of the penis. Obliquely rising extensions approach the anterior superior iliac spines and then are continued directly posteriorly just inferior to the iliac crests. After the umbilicus is encircled, transverse lines are directed laterally toward the lateral costal margins. The skin between the two lateral lines along the midlateral torso is gathered together under tension. With forceful push-up from the lateral buttocks, the lower posterior incision line is continued obliquely over the iliac crest ending up as a rising paramedian line. Through a tissue-gathering maneuver, the superior incision line over the flanks runs along the posterior costal margin.
The marking for the boomerang correction must account for correction of the gynecomastia, superior repositioning of the NACs, removing excess skin of the anterior chest, and effacement of the IMF. The boomerang pattern correction of his gynecomastia wraps around his NACs and then extends in a J shape along the lateral chest to end in each axilla. The position of the receiving domes for the NACs lay several centimeters superior to the inferior lateral adherences of the pectoralis major muscles. The width of these ellipses is adjusted by gathering the skin to remove all excess skin of the medial chest. The lateral oblique ellipse is similarly drawn at roughly right angles to the medial ellipse, except the inferior lateral end is left open for continuation into the J torsoplasty. The J torsoplasty is planned to tighten both the lax back and the anterior chest skin. With the lateral back skin pushed anterior until the laxity is gone, a midlateral chest vertical is drawn. That vertical line is connected to the inferior line of the lateral ellipse. With that line pushed, the width of resection of the C portion resection of the J torsoplasty is determined. After all the lines are drawn, all three crisscrossing ellipses are gathered together to test feasibility of resection.
The operation starts prone for excisions of the oblique flank extensions of the abdominoplasty. Prone followed by supine positioning facilitates twoteam surgery. A two-team approach is preferred and probably obligatory to reduce the time of surgery for a lengthy total body lift. The operating surgeon leads the first team and supervises the second team. The operator for the second team, who has previously assisted the surgeon, watches the first 10 minutes of the opposite side and then makes his incision. The second team working 10 minutes later than the first is most efficient. That delay coupled with continuous communication encourages a symmetrical result in breadth and depth of resection as well as closure. Through several nick incisions, saline with xylocaine and epinephrine is generously infiltrated about the incisions and deeply over the lumbodorsal fascia of the two excision sites.

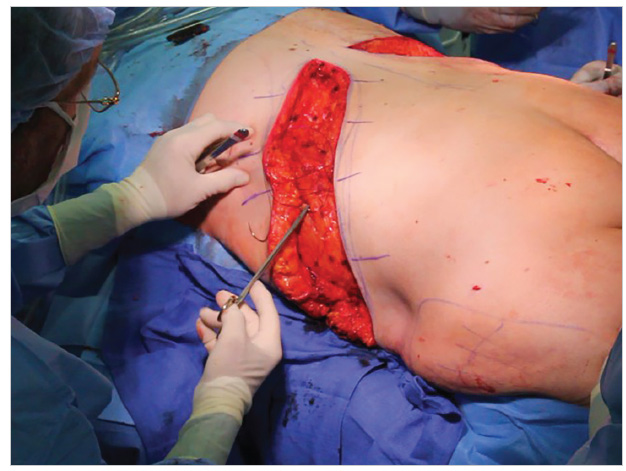
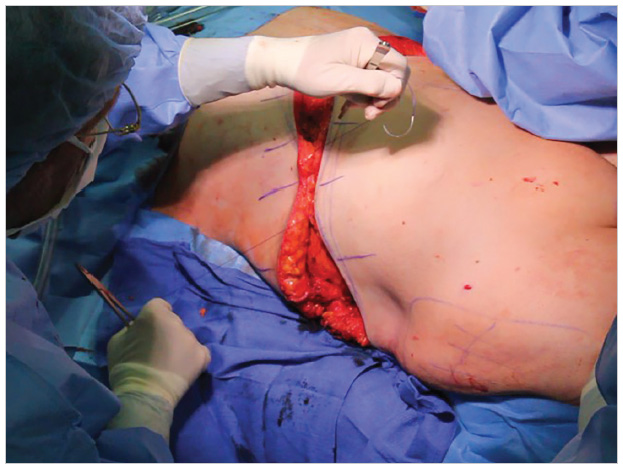
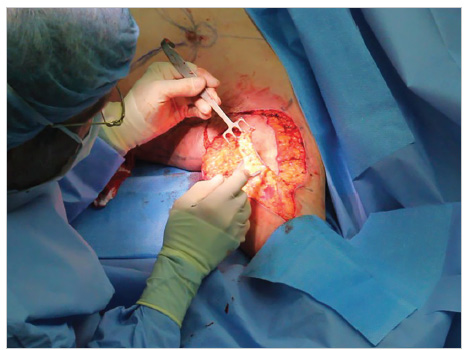
The surgeon incises the inferior markings of the obliquely oriented flank excision first ( Fig. 40.4a ). The inferior skin incision is sharply made with the scalpel and then completed through the highly vascular subdermal tissue with electrosurgery. Then the scalpel cut resumes through the first Scarpa’s fascia layers. The medial portion of the incision is continued by electrosurgery to the lumbodorsal fascia. The midportion of the incision is continued vertically through the tightly packed fat. When the bulging globular gluteal fat is reached, the incision deepens obliquely cephalad through this fat until reaching the lower lumbodorsal fascia ( Fig. 40.4b ). The most lateral third of the incision about the posterior superior iliac spine continues vertically to the fascia overlying the recognizable coarse muscle fibers of the external oblique muscle. Once that incision is complete, the mobile tissue of the buttocks can be pushed cephalad to confirm placement of the markings for the superior incision ( Fig. 40.4c ). The superior incision along the costal margin is a reliable anchor line that holds its position despite a high-tension closure to the inferior flap.
The superior incision is taken vertically down to lumbodorsal fascia over the latissimus dorsi muscle and then skims over its lateral margin to traverse the external oblique ( Fig. 40.5 ).
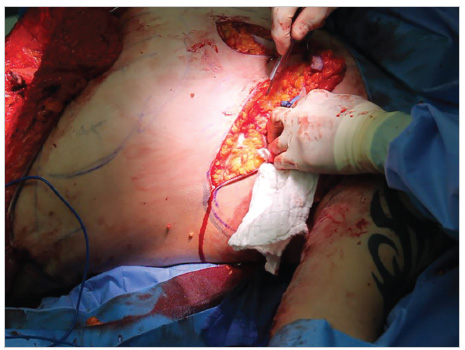
Once the perimeter incision is completed, the resection of the excision site is begun from posterior to lateral ( Fig. 40.6a ). As the excision plane is taken directly over the lumbodorsal fascia to the external oblique, the resection thickness progressively widens to end at the lateral torso at the operating room table ( Fig. 40.6b ). Usually, the resection is completed by electrosurgical cut from the dermal side. Preliminary epinephrine infusion and electrocautery as you go keep blood loss to under 100 mL per side. The surgeon periodically observes the progress of the opposite side team, guiding them through a symmetrical resection. To demonstrate the incredible size and symmetrical thickness of the flank excisions, the two resection specimens are laid out with a 16-cm ruler ( Fig. 40.6c ).
To facilitate closure of this cavernous wound, the operating room table back is elevated. The first of two-layer closure is the superficial subcutaneous tissue with No. 2 PDO Quill 72-cm-long barbed suture on double-armed 48-mm tapered half circle needles. This running suture rapidly encircles the superficial two layers of easily identifiable Scarpa’s fascia on the inferior side of the wound, intervening bits of underlying muscular fascia and all layers of Scarpa’s fascia on the superior (chest) side ( Fig. 40.7 ). This suture technique has multiple goals. By grasping only, the superficial subcutaneous fascial layers, the upper subcutaneous tissue glides over the deep and immobile gluteal fat pad, thereby leaving a subtle tapering approximation down to muscular fascia along the constructed narrow waist. The three-point closure also collapses the dead space to reduce the risk of seroma. This is a secure closure that slightly everts the dermal edges, which facilitates intradermal second layer suturing.



For the entire length of the Quill, 48-mm needles are used to take full-thickness vertical bites that are closest to the dermis, the furthest the bite is away from the wound edge. Starting in the center of the gaping wound, the 48-mm half circle needle is fully passed along the subdermis to almost snag it before turning back through the wound edge ( Fig. 40.7 ). It then enters the opposite wound edge just deep to the top layers of superficial fascia, encircles the fascia, and exits under the dermis. The stitch is slightly pulled to sight the line of closure along the lumbodorsal fascia. Then, two separate wound bites including muscular fascia on either side of the first are taken. Then, the ends are pulled parallel to the closure to fully cinch close to the center of the deep wound ( Fig. 40.8 ). Proper needle placement everts the dermal wound edges and leaves serial pinpoint depressions on either side of the closure. The 72-cm-long double-armed suture is long enough to complete the closure.
The second layer of wound closure is completed through the dermis with 2–0 Monoderm. The patient is then turned supine for abdominoplasty, boomerang correction of gynecomastia, J torsoplasty, and L brachioplasty.
With confidence in the second team surgeon, the lead surgeon starts one brachioplasty, while the second surgeon starts the abdominoplasty ( Fig. 40.9 ). The arms and abdominoplasty are infused with tumescent fluid. After the two-ring VASER probe is applied to the arm excision site, it is handed over to the assistant for the epigastrium.
After the VentX 3.7-mm-diameter aspiration of the excision site is completed, the cannula is handed over to the abdominoplasty surgeon for aspiration of the epigastrium.
Meanwhile, the physician assistant, who will be assisting later in the abdominoplasty, is performing the VASERlipo of the opposite arm (right). When that is completed, he or she will assist the abdominoplasty surgeon, starting the epigastric incision.
After checking the appropriateness of the brachioplasty excision, the L-shaped perimeter incision from the lateral chest across the axilla to the elbow is made. The skin is shave avulsed off the defatted bed of the arm, across the axilla and along the lateral chest to the latissimus dorsi muscle ( Fig. 40.10 ). Electrocautery supplies the limited coagulation of a few bleeders. Gathering the closure together confirms the appropriate width of resection. If there would still be redundant skin, it would have been tangentially excised along the wound margin.

The anchor 2–0 Vicryl stitch is placed through the deltopectoral fascia at the apex of the wound and then through the subcutaneous fascia of the proximal posterior triangular flap and tied.
The arm hemiellipse is set for closure using No. 1 PDO Quill placed in a running horizontal pattern followed by an intradermal 3–0 Monoderm. By then, the assisting surgeon will have completed the VASERlipo of the epigastrium, isolated the umbilicus, and directly undermined a 6-cm-wide path along the epigastrium midline ( Fig. 40.4c ).
Indirect undermining of the remaining epigastrium is through spreading the LaRoe dissectors (ASSI). Then the epigastric flap is pulled down to the planned lower abdominal incision. Because the marked lower incision for the boomerang pattern excision did not move inferiorly by the simulated abdominoplasty closure, that incision can be safely made next.
The incisions through the inferior and posterior boomerang and J torsoplasty patterns are arranged vertically to the thoracic muscular fascia and are made first on the patient’s left and then on the right ( Fig. 40.11 ). Meanwhile, the physician assistant has completed the right L brachioplasty and has gone to assist the second surgeon for the second half of the abdominoplasty. Once it is clear that the undermined epigastric flap can comfortably reach the mons pubis, the lower abdominoplasty incision is made. Across the groins, the incision preserves Scarpa’s fascia for several centimeters of undermining.
Upon completion of the perimeter incision, the lower abdomen skin and subcutaneous tissue are elevated off the premuscular fascia areolar layer. Midline imbrication of a diastasis recti is performed with a double-layered No. 2 PDO Quill. Central high upper abdominal tension is created through three small deepithelialized epigastric dermal flaps within the umbilicoplasty cutout. The flaps at the 3, 6, and 9 o’clock position are sutured to the rectus fascia at the base of the umbilicus with 2–0 Monofilament absorbable.
As the abdominoplasty and umbilicoplasty are being sutured by the second team, the lead surgeon completes the lower and posterior incisions of the upper body lift. After VASERlipo of excessive adipose of the boomerang pattern inferior flap, the inferior chest tissue is discontinuously undermined with gently opening the LaRoe dissector across the IMF to the costal margin, thus stretching and preserving most lower chest perforating vessels.
Once the second team assistant surgeon approximates the abdominoplasty closure, the first team surgeon uses towel clamps to pull up the undermined midthoracic flaps to the marked superior boomerang pattern incision line. The superior and anchor incision line is adjusted as necessary and then incised. The boomerang excision pattern including gynecomastia is then dissected off the pectoralis fascia ( Fig. 40.6c ). Several key stitches position the NAC into the receiving dome.
After a two-layer PDO and Monoderm Quill closure of the boomerang pattern, the surgeon confirms the proper width of lateral vertical chest excision. Incision of the anterior limb of the J torsoplasty completes the perimeter allowing for the cutout. Two-layered barbed suture closes the uneven sides of the J torsoplasty and completes the operation under moderate tension. Imperfections in skin alignment are corrected with fine skin sutures.
Upon completion of the total body lift, improved contours are taut from clavicles to upper thighs with obliteration of the IMF ( Fig. 40.12 ). The results 6 months later were beyond the patient’s expectations ( Fig. 40.13 ).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


