CHAPTER 32 Biceps Augmentation with Silicone Implant
Summary
Biceps augmentation with silicone implant is an option for males who seek to have a more muscular physique. While surgery is not without complications, those who seek a more muscular physique may seek harmful methods such as dangerous dieting and anabolic steroids. While biceps augmentation was initially developed for upper extremity reconstruction of soft-tissue defects secondary to trauma or oncologic surgery, refinements in the surgical technique have facilitated biceps augmentation to advance from a primarily reconstructive procedure to a powerful tool for cosmetic male biceps augmentation. Given the rise of males seeking aesthetic surgery (American Society of Plastic Surgeons shows a 3% increase when comparing 2016 to 2015 and a 28% increase when comparing 2016 to 2000), there will likely be a concomitant increase in males seeking biceps augmentation. In this chapter, we review the pertinent anatomy, preoperative evaluation, operative technique, and postoperative management for biceps augmentation with silicone implant.
Introduction
Biceps augmentation was initially developed for upper extremity reconstruction of soft-tissue defects secondary to trauma or oncologic surgery. In 2006, the use of solid silicone implants for reconstruction of traumatic extremities was reported. 1 Soon after, Chugay et al. 2 reported the use of biceps implants for aesthetic purposes. He had performed 12 biceps augmentations, placing the implant in the submuscular plane. In 2009, Chugay and Chuga. 3 published a retrospective review of 94 cases further describing the procedure as well as the potential risks and complications. All procedures were performed via an incision in the axilla. They reported an increased risk in complications with submuscular placement of the implant compared to subfascial placement. In addition, they noted improved contour with subfascial placement. In 2010, Dini and Ferreri. 4 developed a silicone implant based on the dimensions of the short head of the biceps muscle. The implants were placed via the axilla and in the subfascial plane. Then, in 2012, Abadesso and Serr. 5 reported 32 cases of biceps augmentation using an S-shaped incision in the middle of the arm and placing calf implants into the submuscular plane.
Increased understanding of male aesthetic anatomy, improved implant design, and refinements in surgical technique have facilitated biceps augmentation to advance from a primarily reconstructive procedure to a powerful tool for cosmetic male biceps augmentation.
Physical Evaluation
The Ideal Candidate
Young patient.
Realistic expectations and goals.
Compliant with instruction.
Lean, very little body fat.
Symmetric upper extremity anatomy.
Good skin quality.
No venous insufficiency.
Implant Goals
A natural result.
Undetectable implant borders.
Matches the other muscle groups.
Upper extremity harmony.
Improve Symmetry.
Fill out loose skin envelope.
Physical Examination
Examine the quality of skin and subcutaneous tissue for laxity and fatty deposits.
Evaluate biceps muscle at rest and in flexed position while standing; the proximal and distal portions of the biceps muscle belly are palpated, marked, and measured. These markings determine the maximum length of the implant pocket.
Measure bilateral arm circumference at midportion of arm in flexed, neutral position to determine degree of biceps hypoplasia.
Note any asymmetry and point this out to the patient at the time of examination.
Anatomy
Male upper limb aesthetics are predominantly defined by the shape and development of the biceps and triceps brachii muscles. An anterior and a posterior muscular compartment exist in the upper arm and are separated by the medial and lateral intermuscular septa and humerus. 6 The anterior compartment contains the biceps brachii, brachialis, and coracobrachialis. The posterior compartment contains the triceps brachii muscle. The deep fascia of the arm overlies the biceps and is a continuation of the fascia overlying the deltoid and pectoralis major. Distally, the fascia then becomes the strong intermuscular septa to the medial and lateral aspects that separate the anterior and posterior compartments of the arm.
The biceps has two heads: short and long, which converge into a single unit. The short head of the biceps originates from the coracoid process at the superior aspect of the scapula. The long head originates from the supraglenoid tubercle just above the shoulder joint. The long head has a tendon that passes up along the intertubercular groove of the humerus into the joint capsule of the shoulder joint. The tendon of the short head runs adjacent to the tendon of the coracobrachialis and attaches to the coracoid process. Both heads join on the middle of the humerus, to form a single muscle mass near the insertion of the deltoid, to form a common muscle belly. Distally, the biceps ends in two tendons: the radial tuberosity on the radius and the bicipital aponeurosis, which radiates into the ulnar part of the antebrachial fascia.
While the biceps is typically described as a twoheaded muscle, it has a third head arising from the humerus in approximately 10% of individuals, most commonly originating near the insertion of the coracobrachialis and joining the short head. In addition, the distal biceps tendons are completely separated in 40% and bifurcated in 25% of cases. 6
The brachial artery is the continuation of the axillary artery beyond the lower margin of the teres major muscle and provides major blood supply to the biceps. The venous drainage of the upper extremity is provided by the cephalic vein along with the basilic vein. Fibers of the fifth, and sixth cervical nerves make up the components of the musculocutaneous nerve, which supply motor innervation to the biceps. The lateral antebrachial cutaneous nerve is a continuation of the musculocutaneous nerve and runs in the submuscular region and provides sensory innervation to the skin overlying the lateral arm. This nerve is at risk for injury during submuscular implant biceps augmentation. The medial antebrachial cutaneous nerve is derived from the medial cord of the brachial plexus and provides sensory innervation to the skin overlying the medial arm. The biceps works across three joints: proximal radioulnar, humeroulnar, and the glenohumeral joint. The most important of these functions is to supinate the forearm and flex the elbow.
Steps for Biceps Augmentation
In younger patients or more muscular patients with firmer tissues, it is generally recommended to perform biceps and triceps implantation in a staged manner. This allows the largest implant to be placed while avoiding circulation complications postoperatively, particularly the risk of compartment syndrome.
A helpful strategy is to educate the patient about the value of placing multiple implants, which are not “competing for soft-tissue space.” A typical scenario I discussion with my patients would be as follows:
Stage 1: Biceps, pectoral, medial forearm, medial calf.
Stage 2: Triceps, deltoids, lateral forearm, lateral calf.
Patients tend to appreciate the surgeon’s careful planning, while enjoying the greatest augmentation they can receive, which is appropriate for their soft-tissue envelope.
Implants
Specially designed implants composed of solid silicone, a biologically inert material, are used for biceps augmentation (Alpha Male Aesthetics, Carson City, NV). Given the solid consistency, there is no risk of leakage and systemic dissemination. These implants retain the feel of natural musculature.
Preoperative Markings
Preoperative photographs and videos with the patient flexed and in repose prior to marking are especially helpful to illustrate the asymmetry to the patient. Markings are performed with the patient standing fully upright and the surgeon sitting. In addition to noting the differences between sides and incorporating this into the operative plan, any asymmetry should be pointed out to the patient and clearly documented as many patients are unaware of these asymmetries. While the implant size and/or shape and pocket position should be adjusted to correct asymmetry as best as possible, preoperative identification is paramount to achieving aesthetic success and for managing patient expectations.
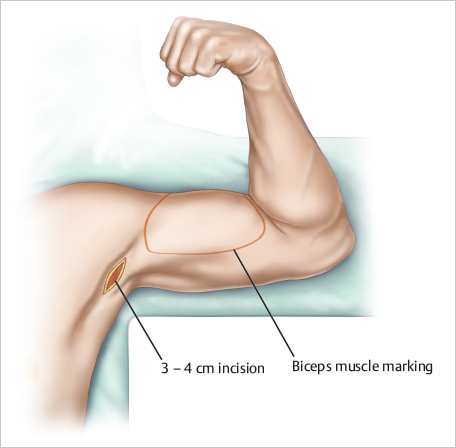
With the arm abducted 90°, the access incision is marked along a natural crease in the axilla ( Fig. 32.1 ). Typically, this incision is 3 to 4 cm long to allow insertion of a folded implant. The biceps contour is then marked out anteriorly and posteriorly with the patient flexed and in repose and additionally with the arm extended. The proximal and distal portions of the biceps muscle belly is palpated and marked. These markings determine the maximum length of the implant pocket. At this point, areas for BodyBanking augmentation and concomitant MuscleShadowing are delineated.
Once all areas of interest have been marked and highlighted, the surgeon should stand up and step a few feet back to assess the overall symmetry. Precise markings translate to operative success and have potential to prevent patient dissatisfaction postoperatively. A final set of photographs and videos with the patient flexed and in repose with the markings are obtained. (See Video 32.1 .)

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


