Case Studies
Introduction
These case studies should be approached after the reader has firmly grasped the aesthetic principles and techniques outlined in the preceding chapters for a more lucid understanding of the content presented herein. Most of this book has been dedicated to a stepwise presentation of how to perform facial fat grafting in an easy and reproducible manner. The title of this book, Complementary Fat Grafting, refers to our strategy of combining fat grafting with ancillary surgical procedures like facelifting and alloplastic implants to enhance overall patient satisfaction. As mentioned previously, this book is primarily intended to provide an explicit description of how and why to perform fat grafting. We do not desire to review other methods of facial rejuvenation, as we believe that the surgeon who is already comfortable with these techniques can implement fat grafting into his or her practice and combine it with existing techniques for facial rejuvenation. This chapter is designed to help that surgeon contemplate how to combine fat grafting in a complementary nature using real case studies for illustrative purposes. For the physician who elects to perform only fat grafting, this book still holds significant relevance, as the techniques outlined in the earlier chapters can be easily accomplished without other surgical intervention.
Case Studies

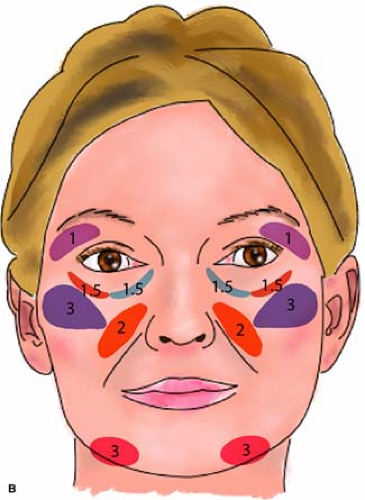 Figure 5-1A: Case Study 1 introduces the complementary approach of combining autologous fat grafting with traditional rejuvenative procedures. The patient underwent a deep-plane rhytidectomy, microliposuction of her jowls, conservative transconjunctival blepharoplasty, and autologous fat transfer. She is shown 13 months postoperatively, with good aesthetic improvement but mild undercorrection of her inferior orbital rim. This case demonstrates the importance of a facelift in achieving the optimal aesthetic result along the jawline for a patient with moderate to marked jowling, which is enhanced by the addition of fat to the prejowl sulcus. Combination of conservative blepharoplasty with autologous fat transfer can optimize the result and minimize the risk of orbital-rim overcorrection. B: Schematic illustration of Case Study 1 shows fat-transfer volumes and distribution with a total of 24 cc of fat: 1 cc to the superior orbital rim, 2 cc to the deep (supraperiosteal) inferior orbital rim, 1 cc to the intermediate depth of the inferior orbital rim, 2 cc to the anterior cheek, 3 cc to the lateral cheek, and 3 cc to the prejowl sulcus. |
History
This 55-year-old woman presented with principal complaints of undesirable lower-eyelid “bags” and prominent jowls. She did not have any significant past medical or surgical history that was contributory.
Consultation
On examination, the patient had good brow position with notable hollowing of her superior orbital rim. Her inferior orbital rim demonstrated mild pseudoherniation of fat in her medial and middle fat compartments, with marked hollowing along the entire length of her inferior orbital rim. She demonstrated a relative flattening of her anterior and lateral cheek. Her jowls were quite pronounced, contributing to an
overall poor contour of her jawline. She also showed significant volume contraction in the prejowl sulcus, which served to exacerbate the appearance of her already heavy jowls. At the time of consultation, the patient was recommended a cervicofacial rhytidectomy, microliposuction of her jowls, and conservative transconjunctival blepharoplasty combined with fat transfer to the volumetrically depleted areas, namely, the superior and inferior orbital rims, the anterior and lateral cheeks, and along her prejowl sulcus.
overall poor contour of her jawline. She also showed significant volume contraction in the prejowl sulcus, which served to exacerbate the appearance of her already heavy jowls. At the time of consultation, the patient was recommended a cervicofacial rhytidectomy, microliposuction of her jowls, and conservative transconjunctival blepharoplasty combined with fat transfer to the volumetrically depleted areas, namely, the superior and inferior orbital rims, the anterior and lateral cheeks, and along her prejowl sulcus.
Intervention
With the above recommendations, the patient underwent a deep-plane rhytidectomy with submentoplasty and microliposuction of her jowls. A conservative transconjunctival blepharoplasty was done to address the lower eyelid medial and middle fat pockets. In addition, she received (per side) 1 cc of fat transferred to the superior orbital rim, 2 cc to the inferior orbital rim in a deep plane, 1 cc to the intermediate depth of the inferior orbital rim, 2 cc to the anterior cheek, 3 cc to the lateral cheek, and 3 cc to the prejowl sulcus on each side of the face.
Results
The patient was very pleased with her aesthetic result. She is shown 13 months after the above procedures with slight undercorrection of her inferior orbital rim, which would benefit from additional fat transfer.
Commentary
Although fat grafting alone along the jawline would have undoubtedly benefited the patient, the heaviness of the jowl mandated a combined approach to achieve the optimal aesthetic result:
The rhytidectomy helped straighten her jawline by elevating the redundant, descended soft tissue of the jowl.
Microliposuction is useful, particularly in a full and heavy jowl.
Fat grafting in the hollow prejowl sulcus can provide improved jawline contouring and obscure the presence of the jowl.
This complementary use of fat grafting in the prejowl sulcus to achieve a straightened jawline has yielded the most uniformly successful results in our hands. Although competing philosophical constructs exist to explain the aging process, gravity versus volume depletion, the question the surgeon should answer is not which mechanism is responsible for aging but how the most likely route toward a successful result can be achieved. Clearly, a rhytidectomy alone can accomplish wonderful aesthetic results. Conversely, pioneers in fat grafting have equally accomplished remarkable benefit in attaining an improved jawline contour with fat grafting alone. In our clinical experience, we have found that combining these approaches can enhance the aesthetic outcome.
Similarly, the patient’s lower-eyelid fullness was most effectively managed through a combination of selective transconjunctival blepharoplasty with fat grafting along her inferior orbital rim. In this patient, the volume loss along the inferior orbital rim and cheek is the more significant problem than actual pseudoherniation of lower-eyelid fat. This is particularly evident on the preoperative photograph of her profile. If an isolated technique were to be used, fat grafting along her inferior orbital rim, transitioning into the cheek, would be much more important than transconjunctival blepharoplasty alone. However, we have found that combining transconjunctival blepharoplasty with targeted fat transfer to the inferior orbital rim has yielded the best aesthetic outcomes. In contrast to this patient, when prominence of the lower-eyelid fat is more a function
of pseudoherniated fat rather than volume depletion, then the importance of blepharoplasty increases proportionately. Considering that most complications in fat grafting occur in the periorbital region owing to either placement of too large a discrete bolus of fat or too much overall volume, judicious lower eyelid fat reduction with blepharoplasty can reduce the volume needed when fat grafting and thereby minimize the risk of complications. The patient at 13 months postoperatively manifests slight undercorrection of her inferior orbital rim, which can be easily corrected with additional fat grafting to this area. Overcorrection of the inferior orbital rim is much more difficult to correct and can be avoided with a conservative approach, as discussed in the previous chapters.
of pseudoherniated fat rather than volume depletion, then the importance of blepharoplasty increases proportionately. Considering that most complications in fat grafting occur in the periorbital region owing to either placement of too large a discrete bolus of fat or too much overall volume, judicious lower eyelid fat reduction with blepharoplasty can reduce the volume needed when fat grafting and thereby minimize the risk of complications. The patient at 13 months postoperatively manifests slight undercorrection of her inferior orbital rim, which can be easily corrected with additional fat grafting to this area. Overcorrection of the inferior orbital rim is much more difficult to correct and can be avoided with a conservative approach, as discussed in the previous chapters.
Although the patient’s original complaint did not concern her relatively hollow cheek region, it was important to discuss with the patient the benefit of fat grafting in this region. Framing the eye concerns not only providing a youthful frame around the eye by supplementing a hollow inferior and superior orbital rim but to think of the cheek as a natural extension of that frame. A fuller, sensuous cheek can accentuate the beauty of the eye. Additional fat in the cheek also carries with it relatively low morbidity, can be rapidly placed, and adds to overall patient satisfaction with the improved facial harmony that is achieved.
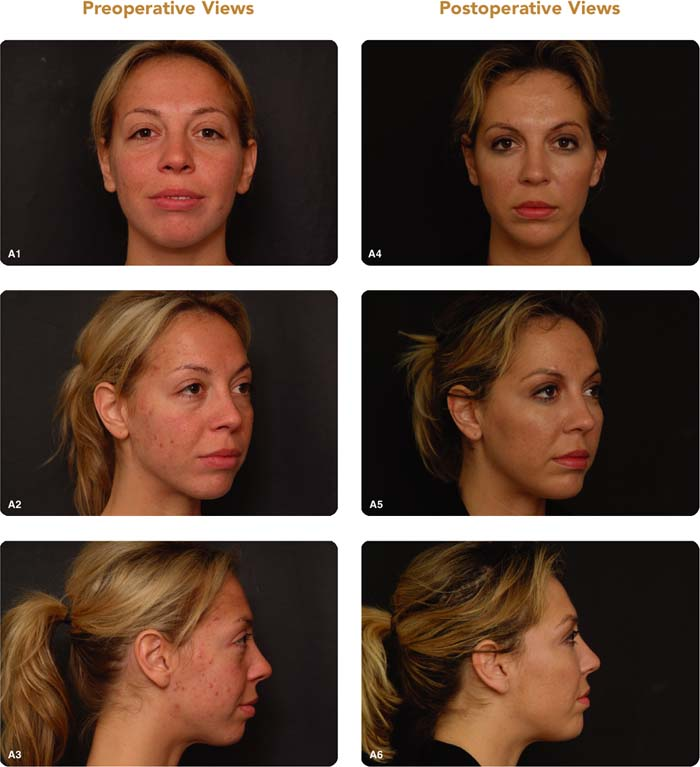
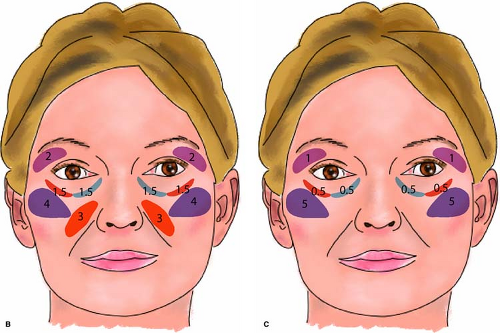 Figure 5-2A: Case Study 2 demonstrates the concept of framing the eye and the benefit of alloplastic implants combined with autologous fat transfer. This patient has a negative-vector eye, mild pseudoherniation of lower-eyelid fat, a retruding superior orbital rim, and microgenia without occlusal malalignment. The negative-vector eye was corrected by increasing the projection of the inferior orbital rim and cheek with fat transfer. A minimal amount of lower medial fat was removed through a transconjunctival approach. Had the lower-eyelid blepharoplasty been undertaken without fat transfer, the procedure would have only exacerbated the prominent appearance of her globe. De-emphasizing her prominent eye also included fat transfer to the superior orbital rim. Although autologous fat transfer can improve a deficient chin, the predictability of adequate projection is less certain than with a standard alloplastic implant. Her microgenia was addressed with a medium-sized extended anatomical silastic chin implant, which gives a more precise and predictable correction than is achieved with fat transfer. B: Schematic illustration of Case Study 2 shows fat transfer volumes and distribution during the first surgery using a total of 24 cc: 2 cc to the superior orbital rim, 2 cc to the deep (supraperiosteal) inferior orbital rim, 1 cc to the intermediate depth of the inferior orbital rim, 3 cc to the anterior cheek, and 4 cc to the lateral cheek. C: Schematic illustration of Case Study 2 shows fat transfer volumes and distribution during the touch-up surgery totaling 14 cc: 5 cc to the lateral cheek, 1 cc to the inferior orbital rim, and 1 cc to the superior orbital rim. |
History
This 35-year-old woman presented with complaints of bulges under her eye and a round appearance of her face. She did not have any significant medical or surgical history.
Consultation
During consultation, the patient was shown that what she perceived as a bulge under her eyes was principally due to the relative hollowing along the inferior orbital rim and
malar region with only minimal fat pseudoherniation in the lower eyelid. More importantly, she exhibited a prominent globe that projected anterior to the superior and inferior orbital rim. A conservative transconjunctival blepharoplasty to remove minimal medial fat with autologous fat transfer to the midface and upper and lower orbital rims improved the appearance of her prominently positioned globe.
malar region with only minimal fat pseudoherniation in the lower eyelid. More importantly, she exhibited a prominent globe that projected anterior to the superior and inferior orbital rim. A conservative transconjunctival blepharoplasty to remove minimal medial fat with autologous fat transfer to the midface and upper and lower orbital rims improved the appearance of her prominently positioned globe.
She also demonstrated moderate microgenia without occlusal malalignment. An alloplastic chin implant provides a more assured method of achieving predictable and precise projection of the mentum than with autologous fat transfer. Correction of her microgenia with a chin implant along with the periorbital and midface fat transfer would yield a more heart-shaped, and feminine face that would also enhance overall facial harmony.
Intervention
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


