55
Carpometacarpal Joint Dislocation
Andrew L. Haas and Kevin D. Plancher
History and Clinical Presentation
A 19-year-old right hand dominant male college student presented to the emergency room with complaints of pain and swelling of his right hand and thumb. He stated that he had injured it 3 months previously in a skiing mogul competition and had an open reduction and internal fixation (ORIF) of his index metacarpophalangeal (MP) joint and proximal phalanx and third MP. He complained of a persistent painful lump on the dorsum of his right thumb. He denied any weakness or numbness.
Physical Examination
The patient was noted to have a dorsal deformity of the thumb with subluxation and instability of the thumb. He had tenderness to palpation with mild weakness secondary to pain. Full active range of motion of the fingers and wrist was intact. Sensation was intact to soft touch. He had 2+ radial and ulnar pulses and less than 2-second capillary refill throughout the hand. He was found to have difficulty with activities of daily living secondary to pain and inability to hold and grab objects.
Diagnostic Studies
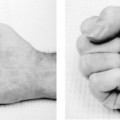
Anteroposterior, lateral, and oblique radiographs of the right hand were obtained. These radiographs revealed a carpometacarpal dislocation of the thumb (Fig. 55–1).

Figure 55–1. (A) Anteroposterior (AP) view of a previously injured hand with dislocated thumb carpometacarpal (CMC) dislocation. (B) Close-up view of dislocated thumb CMC.
Differential Diagnosis
Carpometacarpal joint fracture and dislocation
Metacarpal fractures
Carpal fractures
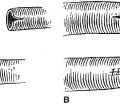
With appropriate radiographic evaluation, the diagnosis of carpometacarpal joint dislocation is rarely mistaken. It is important to rule out associated fractures, as fractures of the bases of the metacarpals are frequently encountered along with this injury (Fig. 55–2). Isolated fractures of the metacarpals and/or the carpus can present with marked generalized swelling with pain and tenderness of the hand. High clinical suspicion needs to be maintained so as not to miss these injuries. Prolonged periods of untreated dislocations have an adverse effect on the future function of the hand and early osteoarthritis.
PEARLS
- Obtain true lateral radiographs to obtain a correct diagnosis.
- Each carpometacarpal joint, when pinned leaves the intermetacarpal ligament intact
- Reduction and stabilization of the third carpometacarpal joint are key to reduction of the remaining carpometacarpal dislocations.
- Attempt closed reduction early, before swelling occurs.
PITFALLS
- Maintain high clinical suspicion of a CMC dislocation to avoid a missed diagnosis.
- Persistent subluxation often presents after closed reduction attempt
- Nonanatomic reduction leads to impairment of mechanical function of the hand.
Diagnosis
Carpometacarpal Dislocation of the Thumb
Carpometacarpal joint dislocations are a relatively rare injury. They are often associated with high-energy trauma or occur as a result of another direct force to the hand, such as in a fall or with punching. The key to making the diagnosis of a carpometacarpal joint dislocation is clinical suspicion. In the event of a high-energy trauma, often other more serious injuries take precedence and the hand injury can be overlooked. In addition, the failure to obtain appropriate radiographs often leads to a failure of diagnosis.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


